Last updated on May 20, 2026
TRICARE TP-2568.6 2014-2026 free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
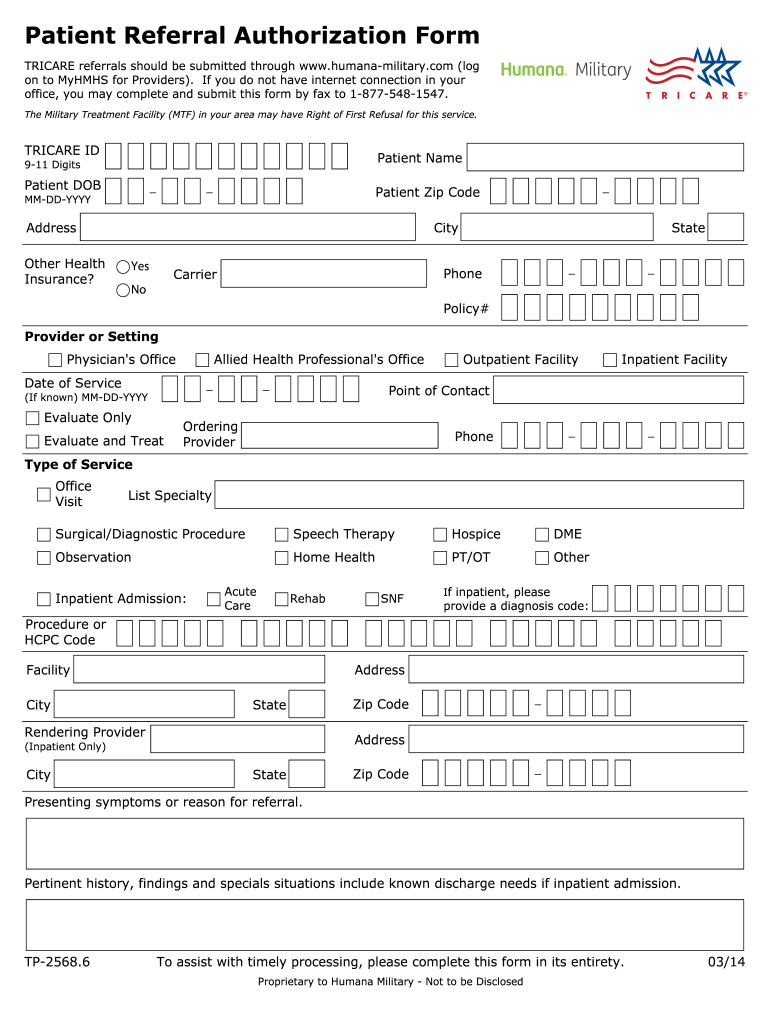
What is TRICARE TP-2568.6
The Patient Referral Authorization Form is a healthcare document used by TRICARE beneficiaries to request medical services from authorized providers.
pdfFiller scores top ratings on review platforms
Who needs TRICARE TP-2568.6?
Explore how professionals across industries use pdfFiller.

TRICARE TP-2568.6 is needed by:
-
TRICARE beneficiaries seeking medical services
-
Healthcare providers referring patients to specialists
-
Military Treatment Facilities processing referrals
-
Medical offices coordinating patient care
-
Insurance representatives managing authorization requests
Comprehensive Guide to TRICARE TP-2568.6
What is the Patient Referral Authorization Form?
The Patient Referral Authorization Form is designed for TRICARE beneficiaries to request medical services efficiently. This form is crucial for accessing necessary healthcare as it facilitates the referral process between patients and providers. Proper completion ensures compliance with healthcare protocols and a smoother transition to necessary medical care.
Purpose and Benefits of the Patient Referral Authorization Form
This healthcare authorization form serves a vital role in obtaining medical referrals from healthcare providers. Utilizing the form streamlines the referral process, making it quicker and more efficient. Benefits include enhanced compliance with healthcare regulations and improved communication between parties involved.
Who Needs the Patient Referral Authorization Form?
The target audience for the Patient Referral Authorization Form includes TRICARE beneficiaries and their healthcare providers. Common scenarios where this form is required include consultations for specialists or when accessing specific medical services under a TRICARE plan.
Key Features and Information Required on the Form
Essential fields included in the Patient Referral Authorization Form are critical for accurate submission. Key elements such as the patient’s name, date of birth, and TRICARE ID must be filled out correctly. The type of service requested and the rendering provider’s details are also vital to ensure that the request can be processed efficiently.
-
Patient Name
-
Patient Date of Birth
-
Patient Zip Code
-
Provider Phone
-
Date of Service
-
Type of Service
-
Rendering Provider
How to Fill Out the Patient Referral Authorization Form Online (Step-by-Step)
Completing the Patient Referral Authorization Form online using pdfFiller involves several straightforward steps. Users can easily navigate through each section of the form to ensure all necessary information is provided accurately.
-
Access pdfFiller and choose the Patient Referral Authorization Form.
-
Fill in patient information, including TRICARE ID and date of service.
-
Provide details for the services requested and the rendering provider.
-
Review the form for any incomplete sections.
-
Save and submit the completed form via online options.
Common Errors and How to Avoid Them
Users frequently make several mistakes while filling out the Patient Referral Authorization Form. These can include missing critical fields or providing inaccurate information. To avoid issues, double-check the form for completeness and accuracy before submission.
-
Ensure all required fields are filled out.
-
Verify the accuracy of patient and provider information.
-
Check for any discrepancies in the service details.
Submission Methods and Delivery Options
After completing the Patient Referral Authorization Form, users have multiple options for submission. Forms can be sent online through pdfFiller or via fax, ensuring a secure method for handling sensitive documents. It’s crucial to consider privacy and security standards when transmitting health information.
After Submission: What to Expect
Once the Patient Referral Authorization Form is submitted, users can expect a response from the Medical Treatment Facility (MTF) within a specific timeframe. It's advisable to check the status of the referral through designated contact methods provided by the MTF.
Security and Compliance for the Patient Referral Authorization Form
Security features of pdfFiller ensure that all documents, including the Patient Referral Authorization Form, are handled with strict data protection measures. Compliance with HIPAA regulations underscores the commitment to maintaining privacy when dealing with sensitive medical documentation.
How pdfFiller Can Help You with the Patient Referral Authorization Form
Utilizing pdfFiller for the Patient Referral Authorization Form simplifies the process of completing, signing, and submitting. Users can enjoy additional features such as easy editing and robust document management capabilities to streamline their experience.
How to fill out the TRICARE TP-2568.6
-
1.Begin by accessing the Patient Referral Authorization Form on pdfFiller. Visit pdfFiller's website and use the search bar to find the form by its name.
-
2.Once the form is open, familiarize yourself with the pdfFiller interface. You may zoom in to read fields clearly and navigate using the toolbar for additional features.
-
3.Gather the necessary information before filling out the form. You'll need the patient's TRICARE ID, name, date of birth, zip code, and details about the requested service.
-
4.Start completing the blank fields. Enter the patient's personal information accurately in the designated sections and ensure correctness.
-
5.Use the checkboxes provided for required selections, such as the type of service and rendering provider. This clarity will aid the processing of the authorization.
-
6.After all fields are populated, review the completed form thoroughly for any errors or missing information. Ensure all necessary details are accurately filled.
-
7.Once satisfied with the information, you can save and download the form directly from pdfFiller. Choose the appropriate file format that meets your requirements.
-
8.To submit the form, follow the specified submission method outlined by your intended provider, whether faxing or uploading electronically, as per their preferences.

Who is eligible to use the Patient Referral Authorization Form?
The Patient Referral Authorization Form is specifically designed for TRICARE beneficiaries seeking to authorize medical services through providers participating in the TRICARE network.
What details are required to complete the form?
Required information includes the patient's TRICARE ID, full name, date of birth, zip code, type of service requested, and provider details to ensure proper processing.
How should I submit the completed form?
Once the form is completed, you can submit it either by fax to the appropriate Military Treatment Facility or electronically, depending on your provider's submission guidelines.
Are there any common mistakes to avoid while filling out the form?
Common mistakes include leaving required fields blank, entering incorrect patient or provider information, and failing to mark checkboxes appropriately. Double-check all entries before submission.
What is the processing time for the referral authorization?
Processing times can vary, but it's typically within a few business days. However, it is advisable to submit referral requests well in advance of any scheduled medical service to allow for adequate processing time.
Do I need to notarize the Patient Referral Authorization Form?
No, the Patient Referral Authorization Form does not require notarization. It should simply be completed, reviewed for accuracy, and submitted as per instructions.
Where can I find additional support if I have questions about the form?
If you have questions regarding the form, you can contact your healthcare provider's office directly or visit the TRICARE website for detailed guidance and resources related to the Patient Referral Authorization Form.
Related Content
Related Forms





Related Catalogs
Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.