Last updated on Apr 3, 2026
Get the free Patient History Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is patient history form
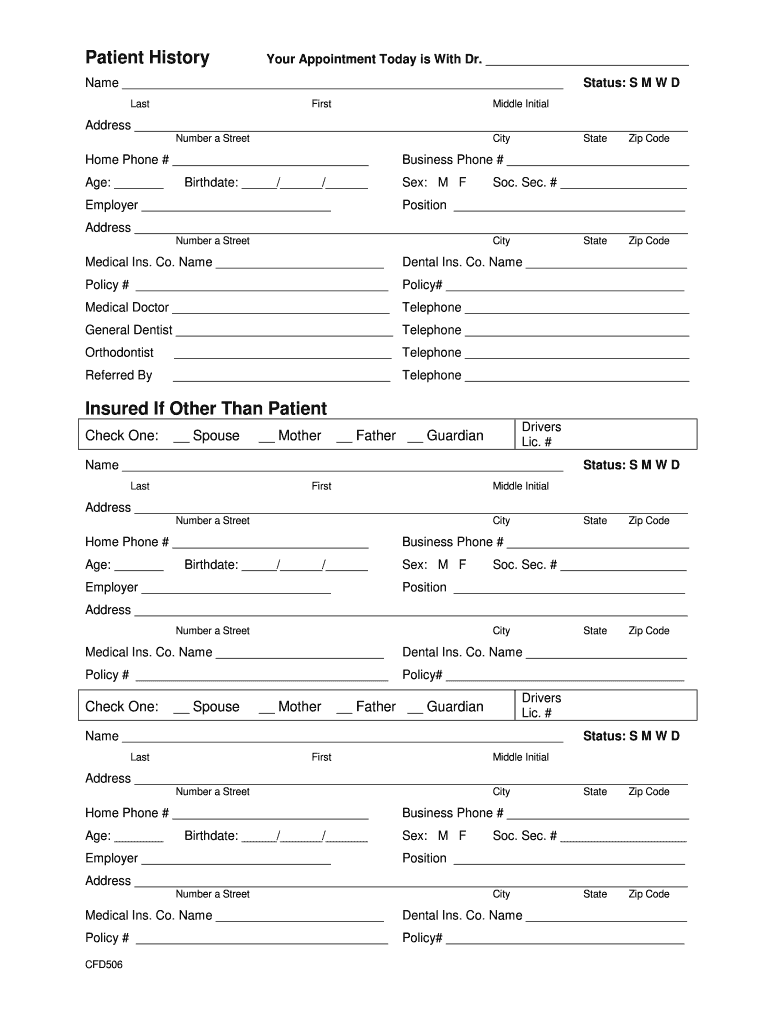
The Patient History Form is a medical document used by healthcare providers to gather essential information about a patient's medical history and personal details.
pdfFiller scores top ratings on review platforms
Who needs patient history form?
Explore how professionals across industries use pdfFiller.

Patient history form is needed by:
-
Patients seeking oral and maxillofacial surgery
-
Guardians completing forms for minors
-
Witnesses required for documentation
-
Insured individuals providing health insurance information
-
Healthcare providers conducting patient intakes
-
Administrative staff managing patient records
Comprehensive Guide to patient history form
What is the Patient History Form?
The Patient History Form is a vital healthcare document that collects essential information about a patient's medical background and personal details. This form is typically filled out by patients or their guardians and is crucial for ensuring accurate medical care. Healthcare providers rely on this form to gather relevant data that assists in diagnosis and treatment planning. Key information collected includes medical history, contact details, and insurance information.
Purpose and Benefits of the Patient History Form
This medical history form is necessary for delivering effective medical care, as it provides healthcare professionals with comprehensive insights into a patient's health. Benefits include improved diagnosis, tailored treatment plans, and better overall patient-provider communication. By streamlining the intake process, the form helps ensure that no critical information is overlooked, ultimately enhancing the quality of care.
Who Needs to Complete the Patient History Form?
Individuals required to complete the patient history form typically include the patient, their guardians, and other authorized persons. Specific roles include:
-
Patient or Guardian
-
Witness
-
Insured Person
Particular attention should be given when minors or dependents are involved, as their guardians will frequently be responsible for filling out the necessary information.
Key Features of the Patient History Form
The Patient History Form includes several critical sections that gather essential details. Important features of the form encompass:
-
Personal details such as name, address, and contact information
-
Medical history including past illnesses and surgeries
-
Insurance details for billing purposes
Additionally, the form requires signatures and authorizations for the release of personal health information, ensuring that all legal and privacy requirements are met.
How to Fill Out the Patient History Form Online (Step-by-Step)
Filling out the Patient History Form digitally using pdfFiller is a straightforward process. Follow these steps to complete the form:
-
Access the form on pdfFiller.
-
Begin with your personal details, ensuring accuracy in every field.
-
Provide your medical and insurance history as required.
-
Review all completed sections for completeness.
-
Submit the form through the platform or save it for later submission.
Accuracy is crucial; double-check that all details are correctly filled to prevent delays.
Common Errors and How to Avoid Them
When completing the Patient History Form, several common mistakes can occur. Frequent errors include:
-
Omitting medical history or insurance details
-
Missing required signatures or authorizations
Before submission, validate the form by reviewing all entries, checking for any potential discrepancies, particularly related to insurance information.
Security and Compliance for the Patient History Form
Handling sensitive patient information requires high-level security measures. The Patient History Form complies with HIPAA regulations to ensure data protection. Using platforms like pdfFiller safeguards user data through 256-bit encryption, ensuring that patient information remains confidential throughout the submission process.
How to Submit the Patient History Form
Submission options for the Patient History Form vary. You can submit the form online through pdfFiller or print it for physical submission. Ensure you send the completed form to the appropriate recipient, such as the healthcare provider or insurance company, and be aware of any deadlines or fees associated with submission.
What Happens After You Submit the Patient History Form?
Upon submission, the Patient History Form undergoes processing and review by the designated healthcare provider. You can expect updates regarding the status of your submission and may need to take follow-up actions depending on the contents of the form. Keeping track of your submission ensures that you address any further requirements promptly.
Experience Seamless Form Filling with pdfFiller
pdfFiller is an ideal solution for completing the Patient History Form efficiently. The platform offers features such as eSigning, document editing, and secure storage. Users can confidently navigate the form-filling process, knowing that their information is handled securely and that the platform is designed for ease of use.
How to fill out the patient history form
-
1.Begin by accessing pdfFiller’s website and use the search function to find the Patient History Form.
-
2.Click on the form to open it in the pdfFiller interface for editing.
-
3.Before starting to fill out the form, gather necessary information such as the patient’s name, address, phone number, age, birthdate, sex, and social security number, along with employment details and insurance information.
-
4.Navigate through the form by clicking on each fillable field to enter the required information, including checkboxes for guardians.
-
5.Utilize the pdfFiller tools to ensure information is entered correctly; you can also edit any mistakes easily by clicking on the text and making changes.
-
6.Once all fields are filled out, review the form carefully to ensure all necessary information has been provided accurately.
-
7.Make sure that all required signatures are added, including those from the patient or guardian, the witness, and the insured person.
-
8.After final review, use the 'Save' option in pdfFiller to store your completed document for future reference.
-
9.You can download the completed form directly to your computer or submit it electronically as required by your healthcare provider.

Who needs to fill out the Patient History Form?
The Patient History Form needs to be filled out by patients, guardians for minor patients, or insured individuals undergoing treatment with healthcare providers, specifically oral and maxillofacial surgeons.
Is there a deadline for submitting this form?
While deadlines for submission can vary by healthcare provider, it is generally recommended to complete the Patient History Form at least a day before the scheduled appointment.
How can I submit the Patient History Form?
You can submit the Patient History Form by downloading it and bringing a printed copy to your appointment, or by using pdfFiller to electronically submit the form directly to your healthcare provider.
What supporting documents are required to complete this form?
Supporting documents are typically not required, but you should have your insurance information handy, including policy numbers and provider details, as well as any relevant medical history information.
What are common mistakes to avoid when filling out the form?
Common mistakes include incomplete fields, missing signatures, and providing inaccurate insurance information. Always double-check your entries before finalizing the form.
What is the processing time for the Patient History Form?
Processing times may depend on the healthcare provider's policies, but typically, the form will be reviewed during your appointment, and any questions can be addressed at that time.
Can I edit the Patient History Form after submitting?
Once submitted, changes can usually only be made by the healthcare provider’s office. It’s best to review the form thoroughly before submission.
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.