
HI HMSA 4000-005 2009-2025 free printable template
Show details
HMSA MEDICAL/DENTAL PLAN ENROLLMENT FORM PLEASE PRINT OR TYPE IN BLUE OR BLACK INK. REFER TO THE BACK FOR ENROLLMENT INSTRUCTIONS. A Group No. Employer EMPLOYEE DATA FOR HMSA USE ONLY Last Name First Legal M. HMSA. com and click on Find a Doctor. SECTION D - OTHER INSURANCE Check Yes to indicate if you your spouse or any of your dependents are also covered by any other group health plan including HMSA or Medicare. If you check Yes enter the other policy holder s name the other policy holder...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign hmsa plan enrollment form
Edit your hmsa enrollment form form online
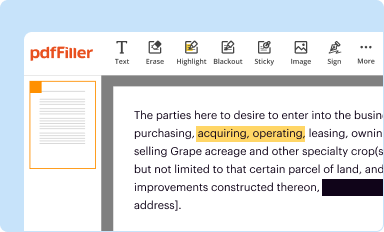
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
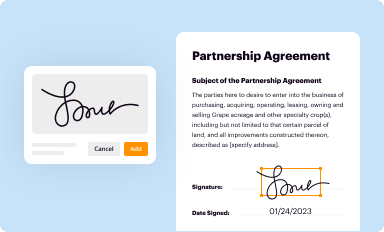
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
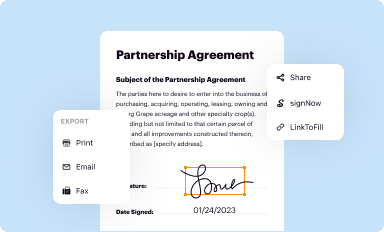
Share your form instantly
Email, fax, or share your hawaii dental form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
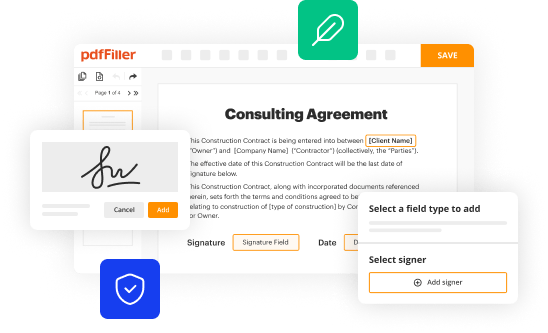
How to edit HI HMSA 4000-005 online



To use the professional PDF editor, follow these steps below:
1
Sign into your account. If you don't have a profile yet, click Start Free Trial and sign up for one.
2
Upload a file. Select Add New on your Dashboard and upload a file from your device or import it from the cloud, online, or internal mail. Then click Edit.
3
Edit HI HMSA 4000-005. Add and change text, add new objects, move pages, add watermarks and page numbers, and more. Then click Done when you're done editing and go to the Documents tab to merge or split the file. If you want to lock or unlock the file, click the lock or unlock button.
4
Save your file. Select it from your records list. Then, click the right toolbar and select one of the various exporting options: save in numerous formats, download as PDF, email, or cloud.
It's easier to work with documents with pdfFiller than you could have ever thought. You can sign up for an account to see for yourself.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out HI HMSA 4000-005
How to fill out HI HMSA 4000-005
01
Obtain the HI HMSA 4000-005 form from the HMSA website or your local HMSA office.
02
Fill in your personal information including your name, address, and contact details in the designated sections.
03
Provide your health plan information and member ID as requested on the form.
04
Clearly mark the type of coverage you are applying for or updating.
05
Review the form for any missing information or errors.
06
Sign and date the form at the bottom where indicated.
07
Submit the completed form to HMSA through the specified method outlined in the instructions (mail, email, or online submission).
Who needs HI HMSA 4000-005?
01
Individuals applying for or updating their health insurance coverage with HMSA.
02
Members of HMSA who need to report changes in personal or health plan information.
03
Families seeking to enroll dependents or changes in their coverage status.
Fill
form
: Try Risk Free
People Also Ask about
Is HMSA considered Medicare?
With HMSA Medicare Advantage, you can get an all-in-one plan with medical, prescription drug, dental and vision, and extra benefits beyond Original Medicare .
Is HMSA a Medicaid?
In Hawaii, most of the Medicaid services are delivered through MCO. There are five (5) MCO health plans: AlohaCare, HMSA, Kaiser Permanente, 'Ohana Health Plan, and UnitedHealthcare Community Plan that provides medical and Long Term Services and Support (LTSS) benefits.
How do I file a claim with HMSA?
If you have a complicated claim question or concern, you can call HMSA's Customer Relations at (808)948-6330 on Oahu or 1(800)790-4672 toll-free on the Neighbor Islands.
What does HMSA stand for medical?
Hawaii Medical Service Association. Menu Employers | Providers Find a Doctor Member Login.
What type of insurance is HMSA?
Medicare Advantage It combines hospital (Medicare Part A), medical (Medicare Part B), and sometimes drug (Medicare Part D) benefits. Insurance companies contract with the federal government to offer Medicare Advantage plans.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I manage my HI HMSA 4000-005 directly from Gmail?
HI HMSA 4000-005 and other documents can be changed, filled out, and signed right in your Gmail inbox. You can use pdfFiller's add-on to do this, as well as other things. When you go to Google Workspace, you can find pdfFiller for Gmail. You should use the time you spend dealing with your documents and eSignatures for more important things, like going to the gym or going to the dentist.
How can I edit HI HMSA 4000-005 from Google Drive?
People who need to keep track of documents and fill out forms quickly can connect PDF Filler to their Google Docs account. This means that they can make, edit, and sign documents right from their Google Drive. Make your HI HMSA 4000-005 into a fillable form that you can manage and sign from any internet-connected device with this add-on.
How can I get HI HMSA 4000-005?
The premium pdfFiller subscription gives you access to over 25M fillable templates that you can download, fill out, print, and sign. The library has state-specific HI HMSA 4000-005 and other forms. Find the template you need and change it using powerful tools.
What is HI HMSA 4000-005?
HI HMSA 4000-005 is a specific form used for reporting health insurance information in Hawaii.
Who is required to file HI HMSA 4000-005?
Entities that provide health insurance in Hawaii are required to file HI HMSA 4000-005.
How to fill out HI HMSA 4000-005?
To fill out HI HMSA 4000-005, you need to provide accurate health insurance policy details, insured member information, and coverage options as specified on the form.
What is the purpose of HI HMSA 4000-005?
The purpose of HI HMSA 4000-005 is to collect data for health insurance compliance and to ensure proper reporting of health insurance details.
What information must be reported on HI HMSA 4000-005?
The information that must be reported includes policy holder details, coverage start and end dates, type of coverage, and any dependents covered under the policy.
Fill out your HI HMSA 4000-005 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
HI HMSA 4000-005 is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
