Last updated on May 2, 2015

Get the free Medical Plan Change Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Plan Change Request
The Medical Plan Change Request Form is a document used by employees to request changes to their Blue Cross group medical coverage.
pdfFiller scores top ratings on review platforms
Who needs Plan Change Request?
Explore how professionals across industries use pdfFiller.

Plan Change Request is needed by:
-
Employees enrolled in Blue Cross group plans
-
HR representatives handling employee benefits
-
Business owners or officers responsible for group medical coverage
-
Employees seeking to switch or update their health plans
-
Healthcare administrators managing employee benefit forms
Comprehensive Guide to Plan Change Request
What is the Medical Plan Change Request Form?
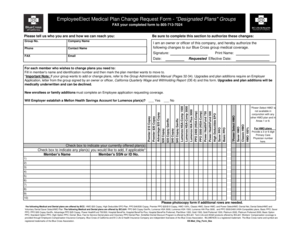
The Medical Plan Change Request Form serves a vital role in facilitating changes to medical plans for members of 'All Plans' groups under Blue Cross coverage. This form is essential for individuals looking to alter their existing health coverage efficiently. Members must utilize this document to ensure their requests are processed smoothly and in accordance with plan regulations.
Primarily, this form is utilized by employees and members who wish to update their medical plan details. The process emphasizes the importance of providing accurate information to avoid any disruptions in coverage.
Purpose and Benefits of the Medical Plan Change Request Form
Submitting the Medical Plan Change Request Form is crucial for several reasons. Firstly, individuals may need to transfer their medical coverage due to changes in employment or personal circumstances. Additionally, updating plan information helps maintain personalized health services and access to necessary care.
Utilizing this form streamlines the entire change process, ensuring that no gaps in care occur during the transition period. Benefits include enhanced continuity of care and simplified management of the medical coverage adjustment.
Key Features of the Medical Plan Change Request Form
The Medical Plan Change Request Form includes several main fields crucial for processing requests. Key features comprise:
-
Group No.
-
Name
-
Phone Number
-
Requested Effective Date
Properly completing each section is essential for successful processing. Accurate entries in these fields minimize delays and enhance the efficiency of the request evaluation.
Who Needs the Medical Plan Change Request Form?
This form is specifically designed for employees and members who are part of 'All Plans' groups. Eligibility criteria dictate that any active employee or covered member can submit a request for changes in their medical coverage. Understanding who is entitled to make these requests ensures the right individuals can access this essential process.
How to Fill Out the Medical Plan Change Request Form (Step-by-Step)
Filling out the Medical Plan Change Request Form requires attention to detail. Follow these steps:
-
Begin by entering your Group No., your Name, and Phone Number.
-
Specify the Requested Effective Date for the change.
-
Fill in your Member’s Social Security or Identification Number.
-
If applicable, indicate whether you want to establish a Health Savings Account for the Lumenos plan.
-
Ensure you sign and print your name, including the date of the request.
-
Review all entries for accuracy before submission.
Proper guidance on these critical sections facilitates a smoother process for the user.
Common Errors and How to Avoid Them
When completing the Medical Plan Change Request Form, common mistakes can lead to processing delays. Some typical errors include:
-
Incorrect or missing Group No.
-
Failure to provide required contact information.
-
Not specifying the Requested Effective Date.
To avoid these pitfalls, always validate all entries thoroughly before submission. Taking the time to double-check can expedite the processing of your request.
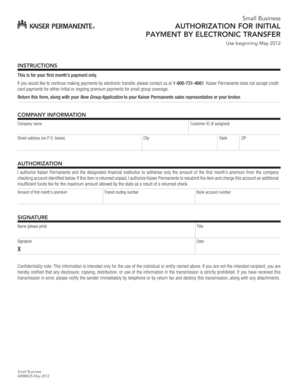
Submission Methods and Delivery of the Medical Plan Change Request Form
Once the form is completed, it must be submitted correctly. The primary method of submission is via fax to a designated number provided in the documentation. Alternative submission methods may be available depending on specific plans.
After submission, users can expect certain processing timelines, which will vary based on request volume and specific circumstances surrounding the change.
What Happens After You Submit?
After submitting the Medical Plan Change Request Form, you will enter the tracking phase of your application. Users can expect feedback within a standard timeframe, which may vary by request type.
Possible outcomes include the approval of changes or a request for additional information. It's essential to stay informed and follow up as needed to ensure desired changes are made.
Security and Compliance in Handling Your Medical Documents
pdfFiller guarantees the security and privacy of sensitive information throughout the submission process. The platform adheres to strict compliance standards, including HIPAA and GDPR, providing users with the confidence that their private data is well-protected.
256-bit encryption and SOC 2 Type II compliance further ensure the safety of your documents during the medical plan change request process.
Maximize Your Experience with pdfFiller for Medical Plan Changes
Enhance your experience by utilizing pdfFiller when filling out, editing, and securely submitting the Medical Plan Change Request Form. This cloud-based solution simplifies document management and ensures easy access to vital features.
Enjoy the benefits of streamlined processes, secure handling, and efficient management of your medical documents with pdfFiller, allowing you to focus on your health needs.
How to fill out the Plan Change Request
-
1.Access the Medical Plan Change Request Form on pdfFiller by searching for the form title in the pdfFiller search bar or by navigating directly to the provided link.
-
2.Open the form by clicking on it within your pdfFiller dashboard to load it into the editing interface.
-
3.Start completing the form by navigating to the fillable fields. Enter your Group No., Name, Phone, and complete each required field carefully.
-
4.Before filling out the Member’s Social Security or ID No. and 6-digit Primary Care Physician number, ensure that you have the necessary information available.
-
5.Indicate the Requested Effective Date for your coverage change in the designated field using the date picker tool.
-
6.Review the sections regarding the establishment of a Health Savings Account. Select 'Yes' or 'No' based on your employer's offerings.
-
7.Add your Signature by clicking in the corresponding field, allowing pdfFiller to either draw your signature or type your name.
-
8.Print your name clearly in the 'Print Name' field and enter the Date of signature completion.
-
9.Double-check all information on the form for accuracy before finalizing. Use the review tool in pdfFiller to identify any missed sections.
-
10.To save your work, click the 'Save' button. For downloading, use the 'Download' option to get a copy of your completed form in PDF format.
-
11.Finally, follow the submission instructions to fax the form to the specified number. Make sure to confirm that it has been sent.

Who is eligible to use the Medical Plan Change Request Form?
Employees enrolled in Blue Cross group plans can use the Medical Plan Change Request Form to request changes to their medical coverage. It's important to confirm that your employer allows such requests.
What information is required to complete the form?
To complete the form, you will need your Group No., name, contact details, Social Security or ID number, Primary Care Physician number, and the desired effective date for your coverage change.
How should I submit the completed form?
Once completed, the Medical Plan Change Request Form must be faxed to the specified number indicated on the form. Ensure that all fields are filled out accurately before sending.
What common mistakes should I avoid when filling out the form?
Common mistakes include leaving required fields blank, entering incorrect identification numbers, and failing to sign and date the form. Always double-check your entries before submission.
Are there any deadlines for submitting the form?
It's essential to check with your HR department for specific deadlines related to the Medical Plan Change Request Form. Timely submission ensures that your coverage change is processed as desired.
How long does it take to process the form once submitted?
Processing times for the Medical Plan Change Request Form can vary. Typically, employers will provide a timeline, but it may take several business days to receive confirmation of the change.
Related Forms




Related Catalogs

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.