Last updated on Apr 10, 2026
Get the free Medicare Prescription Drug Coverage Determination Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is medicare prescription drug coverage
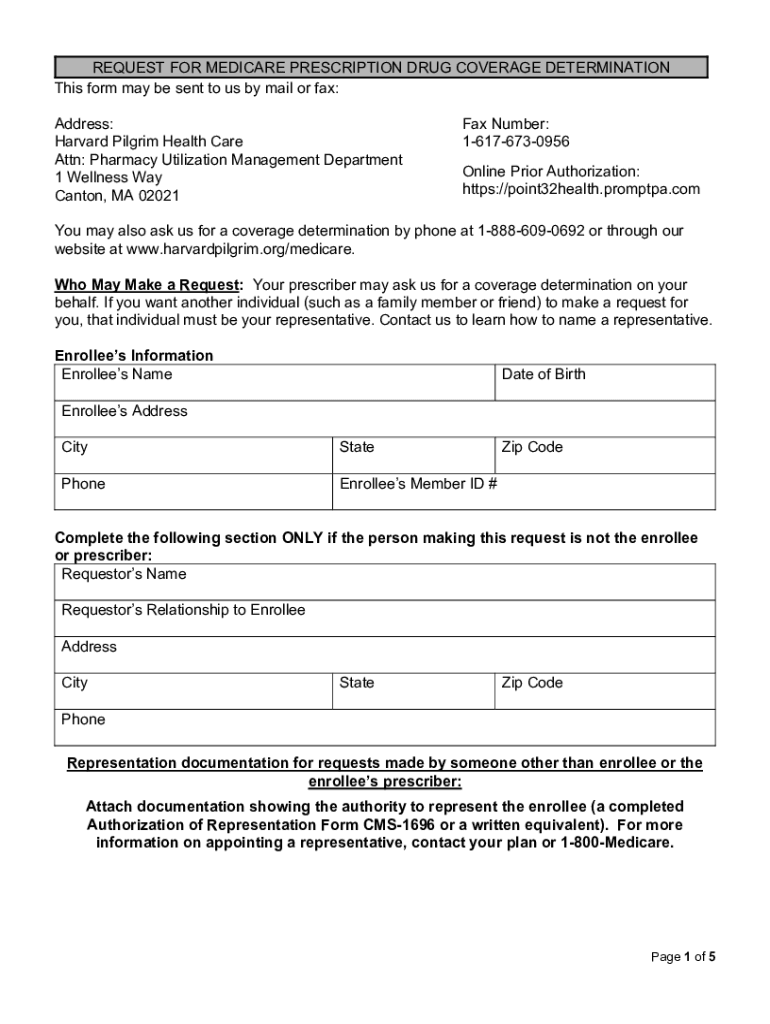
The Medicare Prescription Drug Coverage Determination Form is a medical consent document used by Medicare enrollees to request coverage for prescription drugs from Harvard Pilgrim Health Care.
pdfFiller scores top ratings on review platforms
Who needs medicare prescription drug coverage?
Explore how professionals across industries use pdfFiller.

Medicare prescription drug coverage is needed by:
-
Medicare enrollees seeking drug coverage.
-
Healthcare providers prescribing medications.
-
Patient representatives assisting enrollees.
-
Healthcare administrators managing Medicare forms.
-
Pharmacists verifying coverage options.
Comprehensive Guide to medicare prescription drug coverage
What is the Medicare Prescription Drug Coverage Determination Form?
The Medicare Prescription Drug Coverage Determination Form is a crucial document allowing Medicare enrollees or their representatives to request coverage for prescription drugs. It plays a significant role in facilitating access to necessary medications by enabling enrollees to communicate specific needs to their healthcare providers and Medicare. This form is primarily used by enrollees, requestors, and prescribers to ensure patients receive appropriate drug therapy under their Medicare plans.
Purpose and Benefits of the Medicare Prescription Drug Coverage Determination Form
This form aims to secure necessary prescription drug coverage for those with Medicare. It is particularly beneficial in situations involving formulary exceptions, tiering exceptions, and other unique needs that may require additional steps in the approval process. Expedited requests can also be made in urgent cases where delays could adversely affect the enrollee's health.
Who Needs the Medicare Prescription Drug Coverage Determination Form?
Individuals eligible to use the Medicare Prescription Drug Coverage Determination Form include enrollees, requestors, and prescribers. Various scenarios may warrant its use, such as when an enrollee requires a specific medication not listed on their Medicare formulary or when a prescriber needs to justify a treatment plan that involves higher-cost drugs.
Key Features of the Medicare Prescription Drug Coverage Determination Form
The structure of the Medicare Prescription Drug Coverage Determination Form includes several sections designed for user completion. Key sections comprise enrollee information, drug details, and a prescriber’s statement, each including fillable fields to streamline the submission process. Decisions can also be expedited when necessary, adding flexibility to the approval timeline.
How to Fill Out the Medicare Prescription Drug Coverage Determination Form Online
Filling out the form digitally can significantly simplify the process. Follow these steps to complete the form:
-
Access the online form interface through a compatible browser.
-
Enter relevant information, including the Enrollee’s Name and Date of Birth.
-
Ensure you provide a valid Signature where required.
-
Double-check that all mandatory fields are filled out accurately to avoid delays.
Common Errors and How to Avoid Them
Submitting the Medicare Prescription Drug Coverage Determination Form can be prone to errors. Common mistakes include incomplete fields, incorrect drug information, and missing prescriber statements. To avoid these issues, review the form thoroughly and consult with a prescriber to confirm required information is accurate before submission.
Where and How to Submit the Medicare Prescription Drug Coverage Determination Form
There are several methods to submit the completed form, including online options or traditional mail. Ensure that the completed form is directed to Harvard Pilgrim Health Care, with attention to detail concerning processing times, which can vary. Use confirmation tracking to verify submission status.
Understanding the Aftermath: What Happens After You Submit the Form
Upon submission, the review process for your request begins immediately. Users can check the status of their submission through authorized channels, allowing them to stay informed. Expect communication from either Medicare or Harvard Pilgrim Health Care regarding the decision or need for additional information.
The Importance of Security and Compliance in Submitting Healthcare Forms
When submitting sensitive healthcare documents, maintaining security is essential. Compliance measures, including HIPAA protection, ensure that personal information is handled with care. Users can feel secure knowing that services like pdfFiller utilize rigorous security protocols during the form submission process.
Experience the Ease of Using pdfFiller for Your Medicare Prescription Drug Coverage Determination Form
Utilizing pdfFiller for completing your Medicare Prescription Drug Coverage Determination Form can enhance your experience thanks to its user-friendly interface and advanced functionalities. Features allow for easy editing and secure submission, making it a practical choice for users needing to manage their Medicare forms efficiently.
How to fill out the medicare prescription drug coverage
-
1.Access the Medicare Prescription Drug Coverage Determination Form on pdfFiller by searching for its title in the search bar.
-
2.Open the form within pdfFiller and familiarize yourself with its sections and fields.
-
3.Before filling out the form, gather necessary information including the enrollee’s personal details, prescription drug information, and supporting medical documentation.
-
4.Begin filling in the fields starting with the ‘Enrollee’s Name’ field, followed by the ‘Date of Birth’ and ‘Address’ sections.
-
5.Use the fillable checkboxes to confirm whether certain options apply, ensuring all information is accurate and complete.
-
6.For the prescriber section, obtain a supporting statement from the prescribing doctor to include with the request.
-
7.Review the entire form thoroughly for any missing information or errors before finalizing.
-
8.Once satisfied, save your completed form on pdfFiller either by downloading it as a PDF or submitting it directly as per your needs.
-
9.Follow the submission guidelines provided on pdfFiller to ensure it's sent to Harvard Pilgrim Health Care appropriately.

Who can submit the Medicare Prescription Drug Coverage Determination Form?
The form can be submitted by Medicare enrollees, their authorized representatives, or the prescribing healthcare providers.
What information is required to complete the form?
You will need the enrollee's personal details, prescription drug information, and any relevant medical records or supporting documents.
Is there a deadline for submitting this form?
While the form must be submitted in a timely manner to avoid delays in coverage, specific deadlines can vary based on individual circumstances. Always check with Harvard Pilgrim Health Care for precise timelines.
How can I submit the completed form?
After completing the form on pdfFiller, you can download it for mailing or submit it electronically if that option is available through Harvard Pilgrim Health Care.
What common mistakes should be avoided when filling out the form?
Common mistakes include omitting required fields, providing inaccurate personal details, and failing to attach necessary supporting documents.
What is the processing time for submitted forms?
Processing times for coverage determinations can vary. Typically, it may take up to 72 hours, especially if expedited review is requested due to health concerns.
Are there any fees associated with submitting the form?
Typically, there are no fees for submitting the Medicare Prescription Drug Coverage Determination Form. However, check with Harvard Pilgrim Health Care for any specific policy details.
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.