Last updated on Jun 17, 2015
Get the free Patient Medical History Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is patient medical history form
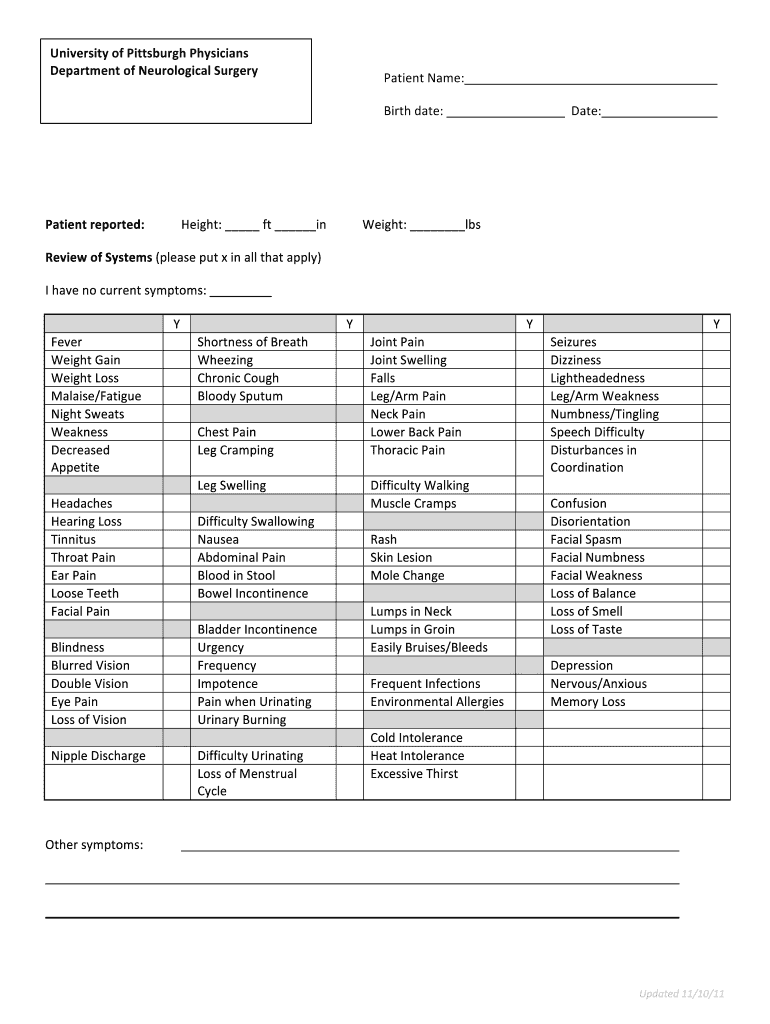
The Patient Medical History Form is a medical document used by healthcare providers to record a patient's medical history and applicable symptoms for neurological assessments.
pdfFiller scores top ratings on review platforms
Who needs patient medical history form?
Explore how professionals across industries use pdfFiller.

Patient medical history form is needed by:
-
Patients seeking neurological evaluations
-
Healthcare providers in neurological surgery
-
University of Pittsburgh Physicians staff
-
Medical professionals conducting patient intake
-
Research teams collecting patient data
Comprehensive Guide to patient medical history form
What is the Patient Medical History Form?
The Patient Medical History Form is a crucial document used in the healthcare sector, particularly by the University of Pittsburgh Physicians Department of Neurological Surgery. This form collects a variety of essential information from patients, including their name, birth date, and specific symptoms they may be experiencing. The comprehensive data gathered through this neurological surgery form plays a significant role in diagnosing and treating various neurological conditions, ensuring that healthcare providers have the information necessary for effective patient care.
Purpose and Benefits of the Patient Medical History Form
The primary purpose of the patient medical history form is to facilitate precise diagnoses by offering detailed accounts of medical histories from patients. Utilizing this healthcare intake form can significantly enhance communication between patients and providers, fostering a more collaborative environment in clinical settings. Additionally, the symptom checklist form aids in supporting efficient treatment planning, allowing providers to tailor their approach based on a comprehensive review of the patient's health.
Key Features of the Patient Medical History Form
This form boasts several key features that enhance its utility for both patients and healthcare professionals. It includes detailed fields for personal information and extensive health symptom checklists. Notably, the structure of the medical history template is designed for ease of use, incorporating checkboxes for common symptoms such as fever and shortness of breath, which simplifies the completion process.
Who Needs the Patient Medical History Form?
The patient medical history form is primarily intended for patients being referred to the University of Pittsburgh Physicians Department of Neurological Surgery. However, it can also be beneficial for other healthcare settings that require a comprehensive neurological history. This form is essential not only for first-time consultations but also for ongoing patient assessments, ensuring that healthcare providers can deliver informed care at every visit.
How to Fill Out the Patient Medical History Form Online (Step-by-Step)
To complete the patient medical history form electronically, follow these steps:
-
Access the form via pdfFiller or the provided link.
-
Fill in your personal details, including name and birth date.
-
Carefully navigate through the symptom checkboxes, marking any that apply.
-
Review your input for accuracy.
-
Submit the completed form according to the provided instructions.
Common Errors and How to Avoid Them
While filling out the patient medical history form, users often encounter a few common pitfalls. Missing fields or failing to correctly check symptoms are frequent errors that can lead to incomplete submissions. To mitigate these issues, double-check all personal information and ensure clarity in the symptoms reported to facilitate accurate assessments.
How to Submit the Patient Medical History Form
There are various methods available for submitting the completed patient medical history form. Options include submitting online via pdfFiller, or printing and mailing the document. After submission, you can expect a confirmation receipt, typically within a few business days, assuring that your information has been processed securely.
The Role of pdfFiller in Completing Your Patient Medical History Form
pdfFiller plays a significant role in simplifying the form-filling process. It offers numerous benefits, including editing and signing capabilities, which enhance the overall user experience. The platform also ensures secured storage and management of sensitive medical documents, making it a practical solution for users needing to complete forms efficiently.
Privacy and Data Protection for Your Patient Medical History Form
When handling sensitive medical forms, privacy is paramount. pdfFiller adheres to HIPAA and GDPR standards, ensuring compliance with legal requirements for data protection. The platform employs 256-bit encryption for secure document handling, allowing users to submit their patient medical history forms with confidence in their confidentiality.
Enhance Your Healthcare Experience with pdfFiller
Utilizing pdfFiller for completing the patient medical history form not only simplifies the process but also enhances the healthcare experience. Consider exploring additional features that support effective healthcare documentation. The convenience of eSigning and document sharing can further streamline your interactions with healthcare providers.
How to fill out the patient medical history form
-
1.To access the Patient Medical History Form on pdfFiller, visit the pdfFiller website and search for the form by its name in the search bar.
-
2.Once you find the form, click on it to open it in the pdfFiller interface where you can start filling it out.
-
3.Before beginning, gather necessary information such as your name, birth date, height, weight, and a list of any applicable symptoms to efficiently complete the form.
-
4.Navigate through the form, filling in the required fields. Click on each blank space to enter information and use the checkboxes to mark any symptoms that apply to you.
-
5.As you fill out the form, make sure all information is accurate and complete. If you need to make changes, you can easily edit the fields at any time.
-
6.Once all necessary fields are filled out, review the form thoroughly to ensure that all information provided is correct and that you have marked any relevant symptoms.
-
7.After finalizing the form, look for options to save, download, or submit it directly from pdfFiller. Choose the method that best suits your needs.

Who is eligible to complete the Patient Medical History Form?
Any patient seeking neurological treatment or evaluation is eligible to complete the Patient Medical History Form. Make sure to fill it out accurately for better care.
What information is required to complete the form?
To complete the form, you will need your name, birth date, height, weight, and a list of relevant symptoms. Having these details handy helps expedite the process.
How do I submit the Patient Medical History Form?
You can submit the Patient Medical History Form through pdfFiller by using the submission options available after completing the form. Ensure your information is accurate before submitting.
What common mistakes should I avoid when filling out this form?
Common mistakes include entering incorrect personal information, overlooking required fields, and forgetting to check relevant symptoms. Double-check your entries before finalizing.
Are there any deadlines for submitting the form?
While specific deadlines may vary, it’s best to submit the Patient Medical History Form as soon as possible to ensure timely evaluation and care from healthcare providers.
Can I save the form for later completion?
Yes, pdfFiller allows you to save your progress. Simply save the form before logging out, so you can easily return to complete it later.
What are the processing times after submitting the form?
Processing times can vary based on the healthcare provider's workload. It's advisable to contact the provider directly for estimated turnaround times after submission.
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.