Last updated on Mar 29, 2026
Get the free Quality Health Family Medical Care Registration Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is quality health family medical
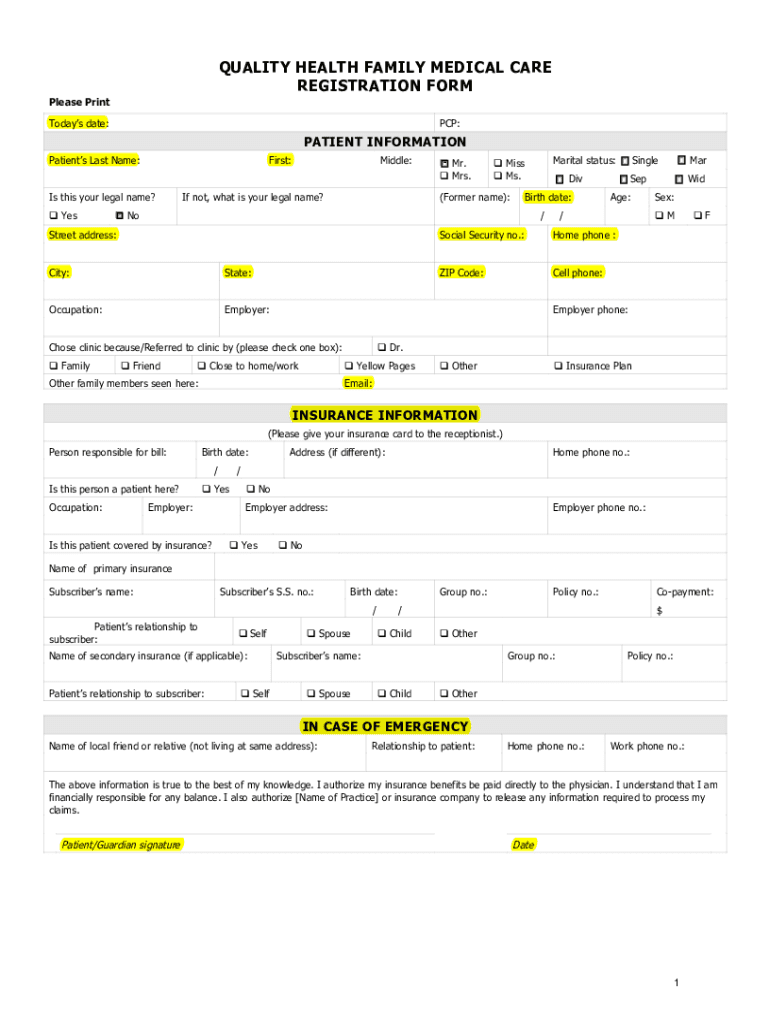
The Quality Health Family Medical Care Registration Form is a healthcare document used by new patients to provide essential information for medical registration and treatment.
pdfFiller scores top ratings on review platforms
Who needs quality health family medical?
Explore how professionals across industries use pdfFiller.

Quality health family medical is needed by:
-
New patients registering at a healthcare facility
-
Guardians filling out medical forms for minors
-
Medical providers requiring patient history and insurance details
-
Insurance companies needing verification of patient information
-
Healthcare administrators managing patient intake processes
Comprehensive Guide to quality health family medical
Understanding the Quality Health Family Medical Care Registration Form
The Quality Health Family Medical Care Registration Form is a crucial document in the patient onboarding process. This form is designed to collect essential patient details, ensuring that healthcare providers have accurate patient data to deliver effective care. Accurate information is vital, as it enables proper diagnosis and treatment planning, minimizing potential medical errors.
This registration form encompasses various types of information, including personal details, insurance information, and medical history. By gathering comprehensive data, providers can tailor their services to meet the unique needs of each patient.
Purpose and Benefits of the Quality Health Family Medical Care Registration Form
The use of the Quality Health Family Medical Care Registration Form offers multiple advantages for both patients and providers. Primarily, it streamlines the registration process for new patients, making it efficient and user-friendly.
Moreover, this form ensures that comprehensive medical history is captured, facilitating better communication between patients and healthcare providers. By providing complete and accurate data, patients can enhance their healthcare experience while aiding providers in delivering informed care.
Key Features of the Quality Health Family Medical Care Registration Form
The form consists of several essential sections tailored to serve user needs. First, it collects personal information, including name, contact details, and emergency contacts. Secondly, it requires insurance details to facilitate billing and claims processes.
Additionally, the medical history section is vital for healthcare providers to understand past medical conditions and treatments. The form is designed with fillable fields for ease of completion and includes clear instructions to guide users through the process. A signature section is included for the necessary authorization, protecting patient privacy throughout.
Who Should Use the Quality Health Family Medical Care Registration Form
This registration form is primarily intended for new patients registering at a medical practice. It is also relevant for guardians who may need to complete the form on behalf of minors or dependents. Moreover, healthcare providers require patients or their guardians to sign the form, authorizing the release of insurance benefits and medical information.
How to Fill Out the Quality Health Family Medical Care Registration Form Online (Step-by-Step)
-
Start by accessing the online version of the Quality Health Family Medical Care Registration Form.
-
Carefully input your personal information in the designated fields, ensuring accuracy.
-
Provide your insurance details, including policy numbers and coverage information.
-
Fill in the medical history section, detailing past medical conditions and treatments received.
-
Review all entered information to confirm its accuracy before submission.
Gather necessary information, such as insurance policy details, beforehand to ensure a smooth filling process. Reviewing your information can prevent errors that may delay your registration.
Common Errors and How to Avoid Them When Filling the Quality Health Family Medical Care Registration Form
When completing the Quality Health Family Medical Care Registration Form, several common errors may arise. These include incomplete fields, incorrect data entries, or omitting required signatures. Such mistakes can lead to delays in processing and may affect your healthcare experience.
-
Ensure all fields are filled in completely.
-
Double-check for accuracy, especially for insurance and personal information.
-
Use a review and validation checklist to verify necessary sections are complete.
Implementing these strategies can help correct errors before submission, enhancing the overall efficiency of the registration process.
Signing the Quality Health Family Medical Care Registration Form: Digital vs. Wet Signature
A signature is a critical component of the Quality Health Family Medical Care Registration Form. It signifies the patient's or guardian's consent and authorization for the release of sensitive medical information and insurance benefits.
There are key differences between digital signatures and traditional wet signatures. Digital signatures provide a secure and convenient option, aligning with compliance requirements such as HIPAA, and ensuring data security during the signing process. Understanding these options can help patients opt for the method that suits them best.
Submission Methods for the Quality Health Family Medical Care Registration Form
Once the Quality Health Family Medical Care Registration Form is completed, there are several methods for submission. Online submission through platforms like pdfFiller is often preferred for its efficiency, while traditional methods, such as mailing or hand-delivery to the office, are also available.
Patients can typically expect a timeline for processing their form, which may vary by practice. It’s crucial to seek confirmation or tracking for your submission to ensure it has been received and is being processed.
Ensuring Security and Privacy When Using the Quality Health Family Medical Care Registration Form
Maintaining security and privacy is paramount when handling sensitive information through the Quality Health Family Medical Care Registration Form. pdfFiller employs robust security measures, including 256-bit encryption and compliance with standards like HIPAA and GDPR.
Patients should be mindful of protecting their personal data when filling and submitting the form. This includes understanding privacy notifications and ensuring proper informed consent regarding the use of their information.
Leverage pdfFiller for Your Quality Health Family Medical Care Registration Form Needs
pdfFiller is an excellent solution for managing the Quality Health Family Medical Care Registration Form due to its user-friendly capabilities. Users can easily edit, fill, and electronically sign their forms to facilitate a smooth registration experience.
With cloud-based access, patients can complete their forms conveniently from any device. pdfFiller offers robust support to users, ensuring that any issues are resolved quickly, further enhancing the overall experience of filling out important healthcare documents.
How to fill out the quality health family medical
-
1.To access the Quality Health Family Medical Care Registration Form on pdfFiller, start by visiting the pdfFiller website and using the search bar to locate the form by its name.
-
2.Once you find the form, click on it to open in the pdfFiller interface. You will see various fillable fields laid out clearly.
-
3.Before you begin filling out the form, gather necessary information such as your medical history, insurance details, and emergency contact information to ensure you have everything ready.
-
4.Navigate through the form by clicking on each field. Enter your information in the designated areas, using the provided checkboxes where necessary.
-
5.If you need to adjust any text, use the editing tools available to modify your responses as needed. Make sure to complete all required fields marked with an asterisk.
-
6.After completing the form, take a moment to review all your entries. Double-check the information to ensure accuracy and completeness.
-
7.Finalize your form by saving your changes on pdfFiller. You can choose to download a copy for your records or submit it directly to the healthcare provider through the platform.
-
8.If you want to submit your form online, follow the submission instructions provided, or print it out to send it by mail or bring it in person during your appointment.

Who is eligible to use the Quality Health Family Medical Care Registration Form?
The form is designed for new patients seeking registration at a healthcare facility. Guardians may fill it out for minors, ensuring accurate information is provided.
Are there any deadlines for submitting this registration form?
It is best to submit the Quality Health Family Medical Care Registration Form prior to your first appointment. Check with the healthcare provider for specific deadlines.
How do I submit the form once completed?
You can submit the form electronically through pdfFiller, download it to send via mail, or bring it in person to your healthcare provider's office.
What supporting documents do I need to provide with this form?
While specific documents may vary, typically you should include your insurance card, photo ID, and any medical records pertinent to your health history.
What are common mistakes to avoid when filling out this form?
Avoid leaving required fields blank, ensure accuracy with your personal information, and double-check your insurance details to prevent processing delays.
How long will it take to process my registration form?
Processing times can vary by provider, but it's typically completed within a few business days. Contact your healthcare facility for specifics.
Can I make changes to my submitted form?
Yes, if you've submitted your form and need to make adjustments, contact the healthcare provider directly to discuss how to update your submitted information.
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.