Last updated on Feb 16, 2015
Get the free Texas Medical Fee Dispute Resolution Request
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
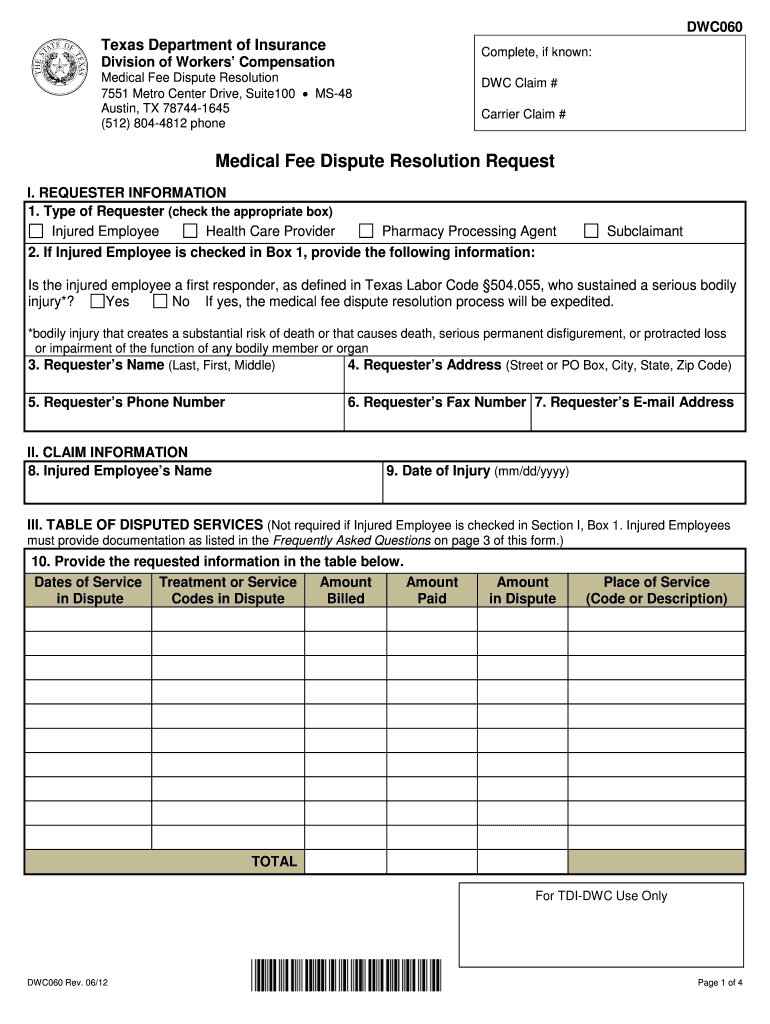
What is Texas DWC060
The Texas Medical Fee Dispute Resolution Request is a legal document used by injured employees and healthcare providers to request resolution of medical fee disputes related to workers' compensation claims.
pdfFiller scores top ratings on review platforms
Who needs Texas DWC060?
Explore how professionals across industries use pdfFiller.

Texas DWC060 is needed by:
-
Injured employees seeking to dispute medical fees
-
Healthcare providers billing for services rendered
-
Employers managing workers' compensation claims
-
Legal representatives for injured employees
-
Insurance adjusters handling claims disputes
-
Medical billers requiring formal dispute resolution
Comprehensive Guide to Texas DWC060
Understanding the Texas Medical Fee Dispute Resolution Request
The Texas Medical Fee Dispute Resolution Request is a vital document aimed at resolving conflicts over medical fees associated with workers' compensation claims. This form enables both injured employees and healthcare providers to formally request resolution when disputes arise. The Texas Department of Insurance, Division of Workers’ Compensation plays a crucial role in processing these requests, ensuring that all parties adhere to the relevant regulations.
In summary, whether you're an injured worker or a healthcare provider, understanding this form is essential for navigating the complex landscape of medical fee disputes in Texas.
Why You Need the Texas Medical Fee Dispute Resolution Request
Resolving medical fee disputes is critical for those involved in workers’ compensation claims. Utilizing the Texas Medical Fee Dispute Resolution Request can lead to timely payments, reducing out-of-pocket costs for employees and providers alike. It is particularly important in scenarios such as billing disagreements or denied claims, where clear and documented communication can expedite conflict resolution.
The form serves as a structured approach to address these issues effectively, enhancing the chances of a favorable outcome.
Who Should File the Texas Medical Fee Dispute Resolution Request?
Eligibility to file the Texas Medical Fee Dispute Resolution Request extends to injured employees, healthcare providers, and employers. Each party has defined roles in this process: injured employees may request resolution for disputed medical fees, while healthcare providers and employers can also initiate filings to dispute unpaid or incorrectly billed services.
Failing to file this request can have significant implications, potentially resulting in increased financial burdens for those who are entitled to compensation.
Gathering Information for the Texas Medical Fee Dispute Resolution Request
Completing the Texas Medical Fee Dispute Resolution Request requires specific information, including personal details and claim specifics. Gather the following necessary documents and supporting materials:
-
Requester’s Name and Address
-
Claims Number
-
Dates of Service
-
Details of the Disputed Services
-
Any Related Correspondence
Accurate information is crucial for ensuring a smooth filing process, reducing the risk of additional disputes or delays.
Step-by-Step Guide on Filling Out the Texas Medical Fee Dispute Resolution Request
Filling out the Texas Medical Fee Dispute Resolution Request can be straightforward if approached systematically. Follow these steps to complete each section of the form:
-
Begin with the Requester’s Name and Address.
-
Provide accurate dates of service and claim numbers.
-
Detail the nature of the dispute clearly.
-
Ensure all fields are completed accurately to minimize errors.
Double-check your entries against the form's instructions to ensure correctness before submission.
Submitting the Texas Medical Fee Dispute Resolution Request
Once the Texas Medical Fee Dispute Resolution Request is complete, it can be submitted in various ways, including online submissions or mailing it directly. Be mindful of deadlines for filing, as late submissions can lead to automatic denials. After submission, tracking your submission status is advisable to stay informed about any developments regarding your dispute.
Common Mistakes When Filing the Texas Medical Fee Dispute Resolution Request
While completing the form, users often encounter typical errors that can hinder the resolution process. Common pitfalls include:
-
Omitting required information
-
Incorrectly filling out specific fields
-
Failing to include supporting documentation
To counter these issues, validate the form against a checklist of essential elements prior to submission, ensuring all areas are correctly filled out.
How pdfFiller Simplifies the Texas Medical Fee Dispute Resolution Request
pdfFiller provides a robust platform for completing the Texas Medical Fee Dispute Resolution Request efficiently. Key features include:
-
Editing capabilities that allow for easy modifications
-
eSigning functionality for secure submissions
-
Cloud access, enabling users to work from anywhere
Moreover, pdfFiller employs strong security measures to protect sensitive data throughout the process.
Next Steps After Submitting the Texas Medical Fee Dispute Resolution Request
After submitting your request, it is crucial to understand the next steps that follow. Typically, you will receive confirmation of receipt, followed by an evaluation of your dispute. Should the matter remain unresolved, you may need to explore further actions, including addressing common rejection reasons by revising your submission based on feedback provided.
Experience Effortless Form Completion with pdfFiller
To streamline the process of filing your Texas Medical Fee Dispute Resolution Request, consider utilizing pdfFiller. The platform’s user-friendly design allows easy access to form editing and management tools. Prioritizing accuracy and security will help ensure that your important documents are handled with the utmost care.
How to fill out the Texas DWC060
-
1.Access the Texas Medical Fee Dispute Resolution Request (DWC Form-060) on pdfFiller by navigating to the website and searching for the form name in the search bar.
-
2.Open the form by clicking on the link provided in the search results, which will open it in the pdfFiller interface.
-
3.Familiarize yourself with the layout of the form, noting blank fields and checkboxes for user input.
-
4.Before starting, gather required information such as the requester's name, address, dates of service, medical codes, and amounts in dispute.
-
5.Begin filling in the form by entering the requester's name and contact details in the designated fields.
-
6.Continue by providing specifics about the dispute, including dates, service codes, and reason for the resolution request.
-
7.Use the fillable table to enter necessary information as guided in the instructions, ensuring accuracy in all entries.
-
8.Once all fields are completed, review the form thoroughly for any missing information or errors to ensure completeness.
-
9.Finalize the form by signing and dating it in the appropriate sections, as this is essential for the request's validity.
-
10.Save your progress frequently and download a copy of the completed form as a PDF using the download button.
-
11.To submit the form, use the provided submission method outlined in your accompanying documentation or submit directly through the Texas Department of Insurance.

Who is eligible to use the Texas Medical Fee Dispute Resolution Request?
This form can be utilized by injured employees, healthcare providers, or entities involved in disputes over medical fees associated with workers' compensation claims in Texas.
What is the deadline for submitting this form?
Though the specific deadline may vary based on individual circumstances, it is generally advisable to submit the dispute resolution request as soon as the fee is contested to avoid delays in processing.
How do I submit the completed DWC Form-060?
The completed Texas Medical Fee Dispute Resolution Request should be submitted to the Texas Department of Insurance, Division of Workers’ Compensation, along with any required supporting documentation.
What supporting documents are needed with the form?
Typically, you will need to include any relevant medical records, bills, and correspondence regarding the dispute. Ensure these documents substantiate your claim for faster processing.
What are common mistakes to avoid when filling out this form?
Common errors include providing incomplete information, failing to include dates and codes accurately, and not reviewing the form before submission. Ensure all fields are filled and double-check details.
How long does it take to process the Medical Fee Dispute Resolution Request?
Processing times can vary; however, it typically takes several weeks. It's advisable to follow up if you haven’t received a response within this timeframe.
What are the consequences of not submitting this form in a timely manner?
Failing to submit the Texas Medical Fee Dispute Resolution Request promptly may result in lost rights to dispute the fees, so it’s critical to act as soon as the dispute arises.
Related Forms


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.