Last updated on Mar 29, 2026
Get the free Patient Demographics Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is patient demographics form
The Patient Demographics Form is a healthcare document used by medical providers to gather essential information about patients for registration and care purposes.
pdfFiller scores top ratings on review platforms
Who needs patient demographics form?
Explore how professionals across industries use pdfFiller.

Patient demographics form is needed by:
-
New or existing patients seeking medical care
-
Parents or guardians of minors requiring healthcare services
-
Healthcare providers needing patient registration documentation
-
Insurance agents verifying patient information
-
Office staff managing patient intake and records
Comprehensive Guide to patient demographics form
What is the Patient Demographics Form?
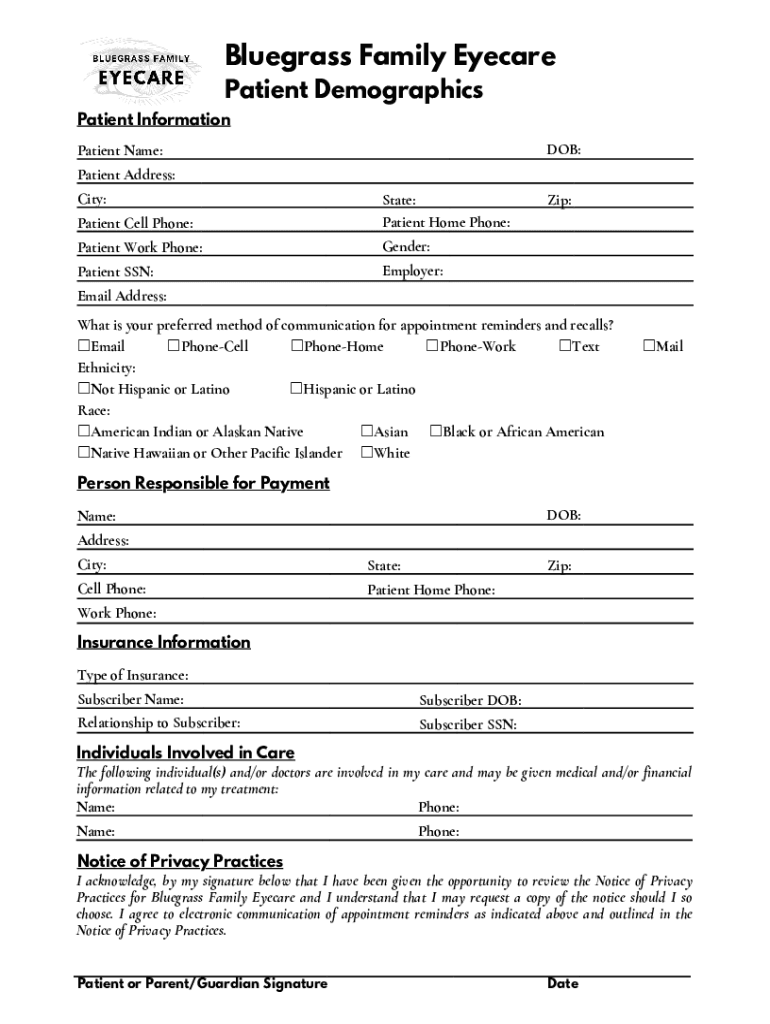
The Patient Demographics Form is a crucial document used in the healthcare sector to gather essential patient information. This form assists healthcare providers in maintaining accurate records, ensuring that they have important details for effective service delivery. Key components of the form include personal details such as the patient’s name, date of birth, and insurance information, all crucial for proper identification and treatment. With terms like "patient demographics form" and "healthcare registration form" being integral to its purpose, the document plays a significant role in the healthcare registration process.
Purpose and Benefits of the Patient Demographics Form
The use of the Patient Demographics Form offers numerous advantages for both healthcare providers and patients. For providers, this patient information form facilitates efficient management of medical records. Patients will enjoy improved coordination of care as a result, making visits to healthcare facilities more seamless.
Some of the core benefits include:
-
Accurate record-keeping for patient history
-
Streamlined communication between healthcare teams
-
Enhanced service delivery during patient visits
Key Features of the Patient Demographics Form
This comprehensive form includes several specific fields to collect essential information. Fillable sections include:
-
Patient Name
-
Date of Birth (DOB)
-
Address
-
Preferred communication methods
-
Ethnic background
Moreover, the form emphasizes security with a signature line, ensuring that privacy acknowledgment is respected, which is paramount in healthcare settings.
Who Needs the Patient Demographics Form?
The Patient Demographics Form is essential for a wide range of users. It is primarily meant for:
-
New patients registering for healthcare services
-
Existing patients needing to update their information
-
Parents or guardians filling out details for minors
Utilizing this form helps ensure that all necessary patient registration & intake information is captured efficiently.
How to Fill Out the Patient Demographics Form Online (Step-by-Step)
Filling out the Patient Demographics Form online can be done easily using pdfFiller. Follow these steps for a seamless experience:
-
Access the Patient Demographics Form on pdfFiller.
-
Enter your details in the designated fillable fields.
-
Select your preferred communication methods.
-
Review the information for accuracy.
-
Sign the form digitally or use a wet signature.
-
Submit the completed form as per the instructions provided.
pdfFiller’s cloud-based platform ensures easy access and enhanced security, making the process user-friendly.
Common Errors When Filling Out the Patient Demographics Form and How to Avoid Them
Many users may encounter common errors while completing the Patient Demographics Form. These errors can result in delays or reprocessing. Common mistakes include:
-
Omitting required fields
-
Incorrect date formats
-
Missing signatures
To avoid these pitfalls, consider using a validation checklist to ensure that all necessary information is complete and accurately filled.
How to Sign and Submit the Patient Demographics Form
Signing and submitting the Patient Demographics Form can be done through several methods. Options include:
-
Digital signatures that meet electronic signature requirements
-
Wet signatures for traditional submission
Once signed, the form can be submitted through pdfFiller or other designated submission methods. You also have the ability to save and download the completed form for your records.
Security and Compliance for the Patient Demographics Form
pdfFiller prioritizes user security when handling the Patient Demographics Form. The platform employs 256-bit encryption and adheres to HIPAA compliance standards, ensuring that sensitive information is protected. This level of security fosters user confidence, knowing that their privacy is respected during the form-filling process.
What Happens After You Submit the Patient Demographics Form
After submitting the Patient Demographics Form, users can expect a typical timeline for processing that may vary based on the healthcare provider's protocols. Follow-ups or confirmations may be sent to inform users of the form's status. Tracking submissions is crucial for maintaining records and addressing any potential issues that may arise post-submission.
Experience Seamless Form Filling with pdfFiller
Utilize pdfFiller to experience the benefits of a user-friendly platform for completing the Patient Demographics Form. Its array of features, such as security measures and easy access, enhance the overall form filling experience, making it efficient and secure.
How to fill out the patient demographics form
-
1.Access the Patient Demographics Form on pdfFiller by searching for it directly within the platform's search bar or by navigating through the healthcare forms section.
-
2.Once the form is open, familiarize yourself with the layout. You'll notice various fields such as 'Patient Name', 'DOB', and sections for contact and insurance information.
-
3.Gather all necessary information before starting. This includes the patient’s full name, date of birth, address, contact number, insurance details, and emergency contact information.
-
4.Begin filling in your details in the respective fields. Click on each textbox to enter information. Use the checkboxes for preferred communication methods and ethnicity/race.
-
5.Review all filled fields to ensure the accuracy of the information entered. Look out for any missing details that might need to be completed.
-
6.Sign the form where indicated, either by using pdfFiller’s electronic signature feature or uploading a scanned signature, if required.
-
7.Once you have completed and signed the form, save your work by clicking the save option. You may also download the completed form directly to your device.
-
8.After saving, choose to submit the form to the appropriate healthcare provider through email or print it for physical submission.

Who is eligible to fill out the Patient Demographics Form?
Anyone seeking medical services, including new patients and parents or guardians of minors, can fill out the Patient Demographics Form. It is essential for registering and managing healthcare records.
Are there any deadlines for submitting this form?
There are usually no strict deadlines for submitting the Patient Demographics Form; however, it is recommended to complete it prior to your first appointment or visit to avoid any delays in care.
How do I submit the completed Patient Demographics Form?
You can submit the completed form via email to your healthcare provider, or by printing it out and delivering it in person. Check with the provider for their preferred submission method.
What supporting documents are needed with this form?
Typically, you may need to provide a copy of your insurance card and a government-issued ID. Check with your provider for any additional documentation required.
What are common mistakes to avoid when filling out this form?
Common mistakes include omitting contact information, inaccuracies in personal details, and not signing the form. Ensure all sections are completed and reviewed before submission.
How long does it take to process the Patient Demographics Form?
Processing times can vary, but typically, forms are reviewed within a few days. For urgent matters, it’s best to follow up directly with your healthcare provider.
What should I do if I have questions while filling out the form?
If you have questions while filling out the form, consult a healthcare staff member for assistance or refer to your provider’s instructions for any specific guidance related to the process.
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.