Get the free California Request for Independent Bill Review
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
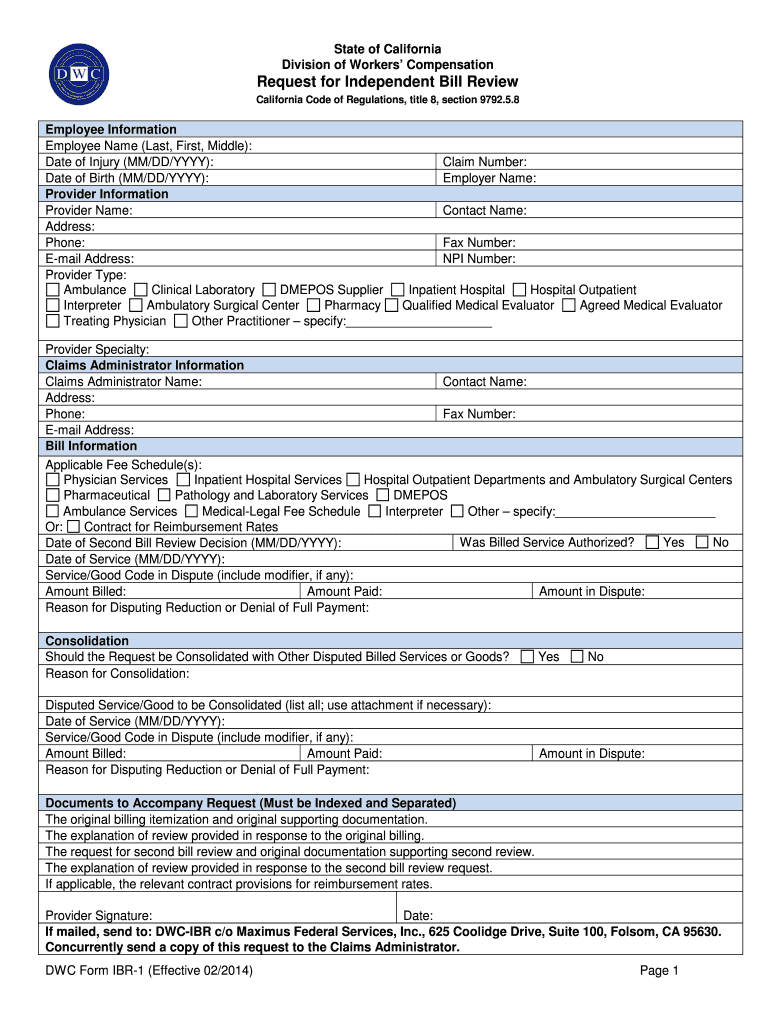
What is CA IBR Form
The California Request for Independent Bill Review is a legal form used by medical providers to dispute payment amounts for workers' compensation medical treatment services.
pdfFiller scores top ratings on review platforms
Who needs CA IBR Form?
Explore how professionals across industries use pdfFiller.

CA IBR Form is needed by:
-
Medical providers challenging payment amounts
-
Claims administrators responding to disputes
-
Legal practitioners advising clients on billing issues
-
Workers' compensation insurers dealing with claims
-
Employee representatives supporting workers' compensation claims
How to fill out the CA IBR Form
-
1.Begin by accessing pdfFiller on your web browser and log in to your account. If you do not have an account, create one.
-
2.Search for the 'California Request for Independent Bill Review form' using the search bar for easy access.
-
3.Once you find the form, click on the 'Edit' or 'Fill' button to open it.
-
4.Familiarize yourself with the form's structure, noting all sections that require your input.
-
5.Gather necessary information including employee details, provider information, and specifics related to the billing dispute, such as service codes and amounts.
-
6.Start filling out the form by entering the required information into each blank field. Use checkboxes where applicable.
-
7.Make sure to include any reasons for disputing the payment reductions or denials clearly in the designated area.
-
8.After completing all sections, review each entry for accuracy and completeness to minimize common errors.
-
9.Use the preview option in pdfFiller to see what your completed form will look like before finalizing.
-
10.Once satisfied with your form, you can save it to your pdfFiller account or download it directly to your computer.
-
11.To submit your form, follow the submission guidelines provided on pdfFiller. Ensure you pay the required fee of $335.00 if applicable, and keep a copy for your records.

Who is eligible to use the California Request for Independent Bill Review?
This form is intended for medical providers who wish to dispute payment amounts under workers' compensation claims in California. Providers need to ensure that they have the necessary details of the billing dispute when filing.
What is the deadline for submitting this form?
The California Request for Independent Bill Review must be submitted within 30 days of the claims administrator's final determination. It's important to adhere to this timeline to ensure your dispute is considered.
How can I submit the completed form?
Once completed, you can submit the California Request for Independent Bill Review through the guidelines specified in the form itself or via pdfFiller. Make sure to include the payment fee of $335.00.
What supporting documents are required for this form?
You will likely need to attach relevant documentation regarding the services provided, billing statements, and any correspondence related to the payments being disputed. Ensure you collect these documents beforehand.
What are common mistakes to avoid when filling out this form?
Common mistakes include entering incorrect service codes, omitting required fields, and missing the submission deadline. Carefully review the form to ensure all required information is complete and accurate before submission.
What are the processing times for an Independent Bill Review request?
Processing times can vary, but typically you should expect a response from the claims administrator within a standard time frame as outlined by California workers' compensation regulations.
Is notarization required for this form?
No, notarization is not required for the California Request for Independent Bill Review, making the process quicker and more accessible for medical providers.
Related Forms


Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.