Last updated on Jun 29, 2015
Get the free Provider Adverse Incident Reporting Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
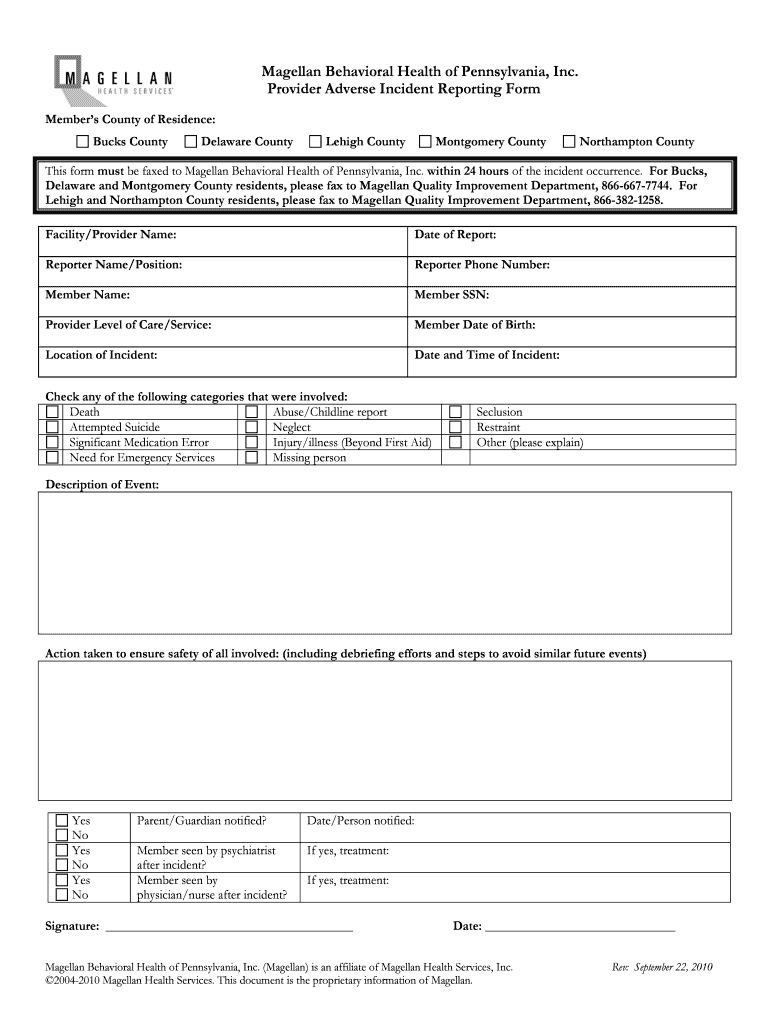
What is Adverse Incident Form
The Provider Adverse Incident Reporting Form is a healthcare document used by providers in Pennsylvania to report adverse incidents involving members.
pdfFiller scores top ratings on review platforms
Who needs Adverse Incident Form?
Explore how professionals across industries use pdfFiller.

Adverse Incident Form is needed by:
-
Healthcare providers in Pennsylvania
-
Medical staff responsible for incident reporting
-
Compliance officers within healthcare facilities
-
Members of Magellan Behavioral Health
-
Legal representatives for healthcare entities
Comprehensive Guide to Adverse Incident Form
What is the Provider Adverse Incident Reporting Form?
The Provider Adverse Incident Reporting Form is a vital document used by healthcare providers in Pennsylvania to report adverse incidents. This form is specifically designed for healthcare providers to submit reports on incidents that adversely affect patients or members. Ensuring submissions are made within 24 hours is crucial for compliance and patient safety.
-
Definition: This form is a structured way for healthcare professionals to document and report incidents.
-
Intended Use: It's utilized primarily by healthcare providers reporting adverse incidents.
-
Submission Timeframe: Reports must be submitted within a 24-hour window of the incident.
Purpose and Benefits of the Provider Adverse Incident Reporting Form
The significance of the Provider Adverse Incident Reporting Form lies in its role in enhancing patient safety and healthcare quality. Timely reporting through this form can lead to improved compliance with healthcare regulations and supports the management and resolution of incidents effectively.
-
Importance of Timely Reporting: Crucial for ensuring patient safety and enhancing care quality.
-
Compliance Benefits: Helps maintain adherence to healthcare regulations.
-
Incident Management: Contributes to more effective protocols for incident resolution.
Who Needs the Provider Adverse Incident Reporting Form?
This form is essential for healthcare providers in Pennsylvania who are mandated to report adverse incidents. Understanding the roles and responsibilities of reporters is key to ensuring accurate and timely submissions.
-
Healthcare Providers: All providers in Pennsylvania are required to utilize this form.
-
Roles of Reporters: Individuals responsible for completing and submitting the form must be aware of their obligations.
-
Situations for Filing: Examples include incidents such as medication errors or patient falls.
How to Fill Out the Provider Adverse Incident Reporting Form Online
Completing the Provider Adverse Incident Reporting Form online is straightforward when following a few key steps. Here’s a guide to assist users in filling out the form accurately.
-
Access the form online through your preferred platform.
-
Fill out critical fields, including member information and incident description.
-
Utilize tools such as pdfFiller to enhance the form-filling experience.
Common Errors and How to Avoid Them
When completing the Provider Adverse Incident Reporting Form, users often encounter common pitfalls that can lead to delays in processing. Avoiding these errors is essential for ensuring accurate submissions.
-
Missing Signatures: Ensure all required signatures are included.
-
Incorrect Information: Double-check all fields for accuracy.
-
Completeness: Confirm that every section of the form is filled out properly.
Submission Methods and Delivery of the Provider Adverse Incident Reporting Form
After completing the form, submitting it in a timely manner is crucial. There are various methods of submission healthcare providers can utilize.
-
Fax Submission: Forms can be faxed directly to Magellan Behavioral Health.
-
Adherence to Timelines: Submission should align with the specified 24-hour guideline.
-
Contact Information: Providers should have contact details handy for follow-up inquiries regarding submission status.
What Happens After You Submit the Provider Adverse Incident Reporting Form?
Following the submission of the form, there are standard procedures that healthcare providers should expect. Understanding these processes can prepare providers for the next steps.
-
Responses from Magellan Behavioral Health: Providers can anticipate specific timelines for feedback.
-
Expected Actions: Be prepared for additional follow-up requests or informational needs.
-
Amendments: Information on how to amend submissions if corrections are necessary will be provided.
How pdfFiller Can Assist You with the Provider Adverse Incident Reporting Form
pdfFiller offers powerful features to facilitate the completion of the Provider Adverse Incident Reporting Form, ensuring a streamlined process.
-
Editing Capabilities: Users can easily edit text and images within the form.
-
eSigning Features: Secure eSigning options are available for added convenience.
-
Security Assurance: PdfFiller is HIPAA compliant, ensuring the protection of sensitive information.
Sample Provider Adverse Incident Reporting Form
Having a reference sample of the Provider Adverse Incident Reporting Form can greatly assist users in understanding proper completion techniques. Below are some key features of the sample form.
-
Completed Form Example: A filled-out form serves as a template for users.
-
Annotations Included: Important areas of the form highlighted for clarity.
-
Template Availability: Users can access templates through pdfFiller for ease of use.
Engage with pdfFiller for Smooth Form Completion
Utilizing pdfFiller can greatly enhance the efficiency of filling out and submitting the Provider Adverse Incident Reporting Form. This platform not only simplifies the process but also ensures accuracy in submissions.
-
Importance of Accuracy: Emphasizes the need for precise reporting in all healthcare documentation.
-
Convenience Features: Highlights how pdfFiller enhances productivity during form completion.
-
Encouragement to Start: Users are invited to begin the form completion process with the help of pdfFiller.
How to fill out the Adverse Incident Form
-
1.To access the Provider Adverse Incident Reporting Form on pdfFiller, visit the pdfFiller website and use the search bar to locate the specific form by name.
-
2.Once located, click on the form to open it in the pdfFiller interface, which allows you to edit and fill out the document directly.
-
3.Before you begin filling the form, gather all necessary information about the incident, including the member's information, description of the incident, actions taken, and any notifications made.
-
4.Using pdfFiller’s tools, click on each blank field and enter the required data, making sure to complete all necessary sections, paying close attention to the clarity of your input.
-
5.As you fill in the fields, use the clear instructions provided within the form to ensure that all blank spaces are appropriately addressed and compliance is met.
-
6.After completing the form, take a moment to thoroughly review all entries for accuracy and completeness. Ensure that all required signatures are present.
-
7.Once satisfied with the content, use pdfFiller's download or submission options to save your form. You can also fax the completed form directly to Magellan Behavioral Health as required.

Who is eligible to use the Provider Adverse Incident Reporting Form?
The form is specifically designed for use by healthcare providers and medical staff in Pennsylvania reporting adverse incidents related to their members.
What is the submission deadline for this form?
The completed form must be faxed to Magellan Behavioral Health within 24 hours of the incident to ensure timely processing and compliance.
How do I submit the Provider Adverse Incident Reporting Form?
Once the form is completed, you can fax it to Magellan Behavioral Health as instructed. Ensure the form is completed correctly before submitting.
What information do I need to fill out this form?
You will need information such as the member's details, incident description, actions taken, and individuals notified of the incident. Make sure all fields are filled out accurately.
What are common mistakes to avoid when filling out the form?
Common mistakes include incomplete fields, missing signatures, and failing to submit the form within the required timeframe. Make sure to double-check all entries.
How long does it take for the form to be processed?
Processing times may vary. However, submitting your form promptly and accurately will help ensure it is processed in a timely manner.
Do I need to notarize the Provider Adverse Incident Reporting Form?
No, this form does not require notarization before submission. Ensure all required signatures are included for validity.
Related Forms


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.