Last updated on Apr 10, 2026
Get the free Health Partners Plans Prior Authorization Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is health partners plans prior
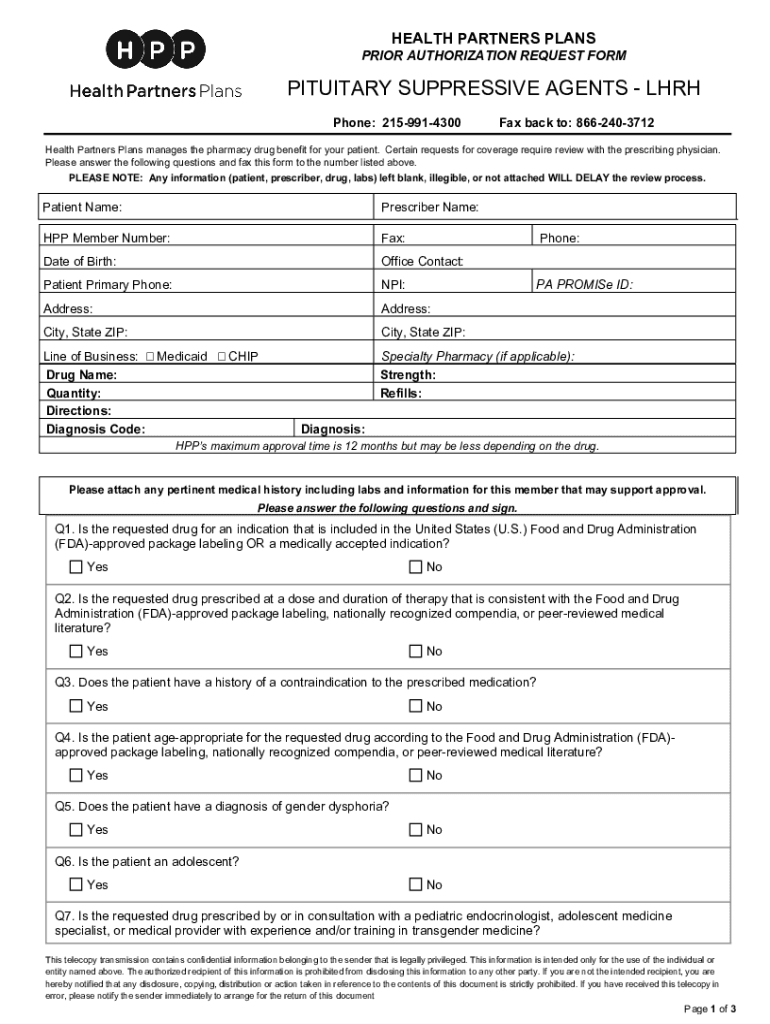
The Health Partners Plans Prior Authorization Request Form is a healthcare document used by prescribers to request prior authorization for pituitary suppressive agents (LHRH) for their patients.
pdfFiller scores top ratings on review platforms
Who needs health partners plans prior?
Explore how professionals across industries use pdfFiller.

Health partners plans prior is needed by:
-
Healthcare providers requesting medication authorization
-
Patients needing LHRH treatments
-
Pharmacies dispensing medications requiring prior approvals
-
Medicaid and CHIP program participants
-
Medical administrators handling authorization requests
Comprehensive Guide to health partners plans prior
What is the Health Partners Plans Prior Authorization Request Form?
The Health Partners Plans Prior Authorization Request Form serves as a critical tool for healthcare providers to secure approval for treatments involving pituitary suppressive agents, specifically LHRH. This form is significant in the healthcare process as it ensures that prescribers can validate the medical necessity of the requested treatments. Exclusively for prescribers, the form requires a signature to authenticate the request before submission.
Purpose and Benefits of Using the Health Partners Plans Prior Authorization Request Form
This form primarily aims to facilitate a smoother approval process for medications, benefiting both healthcare providers and patients. By effectively utilizing the Health Partners Plans Prior Authorization Request Form, prescribers can ensure compliance with insurance requirements and expedite medication authorizations. This streamlining is crucial for meeting medical necessity standards effectively.
Key Features of the Health Partners Plans Prior Authorization Request Form
-
Required fields for patient identification, including name and date of birth.
-
Prescriber information fields such as name, contact details, and credentials.
-
Drug prescription specifics including name, dosage, and quantity requested.
-
Yes/no questions to assess the patient’s medical history and FDA compliance.
-
Explicit instructions for completing and submitting the form.
Who Needs the Health Partners Plans Prior Authorization Request Form?
The primary audience for this form consists of healthcare providers, such as prescribers who possess the necessary qualifications to complete it. These prescribers should have credentials confirming their ability to handle such requests, ensuring accurate submissions that uphold the standards of patient care. Scenarios requiring patients to have a prescriber complete this form typically involve treatments needing prior authorization before medication dispensing.
How to Fill Out the Health Partners Plans Prior Authorization Request Form Online
-
Access the form using an online tool like pdfFiller.
-
Input all required information, ensuring accuracy in the patient and prescriber sections.
-
Pay attention to the specialized fields regarding drug prescription.
-
Avoid common pitfalls like incomplete fields or incorrect drug details.
-
Save the completed form and submit it electronically to the designated channels.
Important Considerations and Compliance for the Health Partners Plans Prior Authorization Request Form
Accurate data submission is crucial for obtaining timely approvals for treatments requested via the form. Inaccurate or late submissions can lead to significant delays or outright denials of medication requests. Furthermore, adherence to security and confidentiality measures during patient information handling is essential to protect sensitive data.
Submission Methods for the Health Partners Plans Prior Authorization Request Form
-
Faxing the completed form directly to Health Partners Plans.
-
Online uploads through verified healthcare platforms.
-
Submission based on jurisdictional requirements, which may vary by state.
-
Awareness of any applicable submission fees and estimated processing timelines.
What Happens After You Submit the Health Partners Plans Prior Authorization Request Form?
After submission, the Health Partners Plans review process begins, where healthcare requests are assessed for appropriateness. Providers can track or confirm their submissions through specified channels. Potential outcomes include approval, denial, or requests for additional information, each of which has its own implications for the patient’s treatment plan.
How pdfFiller Can Help with the Health Partners Plans Prior Authorization Request Form
pdfFiller simplifies the form-filling process by offering a user-friendly interface for editing, signing, and submitting the Health Partners Plans Prior Authorization Request Form securely. It is designed with essential security measures, including 256-bit encryption and compliance with standards like HIPAA, ensuring that users' information remains safe throughout the document management process.
How to fill out the health partners plans prior
-
1.To access the Health Partners Plans Prior Authorization Request Form on pdfFiller, visit the pdfFiller website and use the search bar to find the specific form by entering its name.
-
2.Once the form is located, click on it to open it in pdfFiller's editing interface, where you can view all required fields.
-
3.Before starting to fill out the form, gather necessary patient information such as name, prescriber details, and relevant diagnosis codes to ensure all information is accurate and complete.
-
4.Begin filling in the form by clicking on each blank field. Enter the patient’s name, prescriber’s name, and other required identifiers in the allocated spaces.
-
5.Utilize the checkboxes provided for yes/no questions regarding the patient's medical history and drug compliance. Confirm your choices by clicking the appropriate boxes.
-
6.As you complete each part of the form, refer to any instructions included for guidance, ensuring adherence to deadlines or special requirements.
-
7.After completing all sections, review the form for any errors or missing information to ensure all is in order before submission.
-
8.Lastly, once you are satisfied with the completed form, click the 'Save' option to keep a copy for your records, or use the download feature to save it directly to your device.
-
9.You may also submit the form via fax to Health Partners Plans directly from pdfFiller if this option is available. Otherwise, ensure you print the completed form and send it manually.

Who is eligible to use the Health Partners Plans Prior Authorization Request Form?
The form can be used by healthcare providers who prescribe pituitary suppressive agents (LHRH) for their patients, as long as they meet the necessary criteria of the Health Partners Plans.
Is there a deadline for submitting the prior authorization request?
It is essential to submit the prior authorization request as soon as possible to avoid delays in treatment. Check with Health Partners Plans for specific processing times that may apply.
What is the preferred submission method for the completed form?
The completed Health Partners Plans Prior Authorization Request Form should be faxed to Health Partners Plans as indicated in the form instructions. Ensure you follow any additional procedures for submission.
What supporting documents are required when submitting the form?
Typically, you may need to include patient insurance information, relevant medical records, and any existing treatment documentation alongside the authorization form for smoother processing.
What common mistakes should be avoided when filling out the form?
Be careful to provide accurate patient and prescriber information, ensure all yes/no questions are answered appropriately, and double-check for missing signatures before submission.
How long does processing usually take for prior authorization requests?
Processing times can vary based on the volume of requests received; however, it generally takes several business days. Verify with Health Partners Plans for more specific information.
What should I do if my prior authorization request is denied?
If a request is denied, review the denial letter carefully for reasons. You can appeal the decision by providing additional information or medical justification as directed by Health Partners Plans.
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.