Last updated on Apr 10, 2026

Get the free Patient Information Authorization Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is patient information authorization form
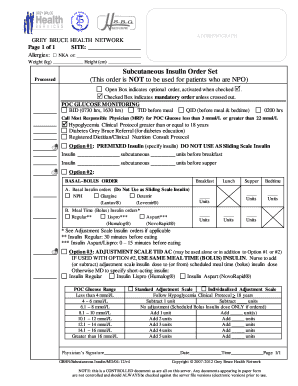
The Patient Information Authorization Form is a medical consent document used by Lexington Women’s Care to collect essential patient details and provide authorizations for treatment and HIPAA privacy practices.
pdfFiller scores top ratings on review platforms
Who needs patient information authorization form?
Explore how professionals across industries use pdfFiller.

Patient information authorization form is needed by:
-
Patients seeking medical care from Lexington Women’s Care.
-
Individuals needing to provide their insurance information.
-
People authorizing Medicare benefits.
-
Anyone requiring HIPAA acknowledgment.
-
Patients undergoing treatment requiring consent.
Comprehensive Guide to patient information authorization form
What is the Patient Information Authorization Form?
The Patient Information Authorization Form is a crucial document used by Lexington Women’s Care in South Carolina to collect essential patient data and authorizations. This form plays a key role in ensuring that healthcare providers can obtain necessary consents while adhering to HIPAA regulations. It requires the patient's signature, signifying their understanding of privacy practices related to their medical information.
Purpose and Benefits of the Patient Information Authorization Form
This healthcare form streamlines the patient registration process, allowing for efficient intake during visits to Lexington Women’s Care. Obtaining informed consent through this form enhances privacy and secures necessary authorizations for sharing medical data. The use of this medical consent form fosters improved communication between patients and healthcare providers, ensuring that everyone involved is well-informed.
Key Features of the Patient Information Authorization Form
The Patient Information Authorization Form includes several important sections designed for user convenience. Major fields encompass personal data, an emergency contact section, and insurance details. The form also contains checkboxes and blank fields to capture information such as language proficiency, making it more accommodating for diverse patients. Its layout prioritizes ease of use, enabling patients to complete the form efficiently.
Who Needs the Patient Information Authorization Form?
Patients visiting Lexington Women’s Care must fill out the Patient Information Authorization Form, particularly during first-time visits or when making insurance claims. This form is vital for compliance with medical regulations, ensuring that all necessary data is gathered and authorized prior to any treatment. Each patient's submission contributes to a seamless healthcare experience.
How to Fill Out the Patient Information Authorization Form Online (Step-by-Step)
-
Access the Patient Information Authorization Form through pdfFiller.
-
Begin filling out the personal data section, including your name and date of birth.
-
Complete the emergency contact and insurance details sections as prompted.
-
Ensure all relevant checkboxes are selected, particularly for consent and HIPAA acknowledgment.
-
Review your entries to avoid common errors before submission.
-
Submit your completed form digitally for processing.
Submission Methods and Delivery for the Patient Information Authorization Form
Patients can submit the Patient Information Authorization Form through multiple channels. Digital submissions via pdfFiller offer convenience, while mailed options are available if needed. After submitting the form, patients can expect to receive confirmation and may be required to follow up on their submissions. Be aware of potential fees or processing times associated with the submission method chosen.
Security and Compliance for Handling Patient Information
Security is paramount when it comes to handling the Patient Information Authorization Form. pdfFiller employs advanced security features, including 256-bit encryption and adherence to HIPAA compliance, ensuring that sensitive patient information is protected. Utilizing a secure platform is essential for maintaining patient confidentiality and trust.
Common Errors and How to Avoid Them When Completing the Patient Information Authorization Form
Completing the Patient Information Authorization Form can lead to mistakes if users are not careful. Common errors include incorrect personal information, missing signatures, and failing to check necessary boxes. Patients are encouraged to double-check their entries and utilize pdfFiller's checks for common issues to enhance accuracy and completeness before submission.
Sample of a Completed Patient Information Authorization Form
A downloadable link or visual representation of a completed Patient Information Authorization Form is available for reference. This sample includes annotations that explain each section and field, enabling patients to better understand what is required. It serves as a helpful guide to refer to while completing your own form.
Get Started with pdfFiller for Your Patient Information Authorization Form
pdfFiller provides an ideal platform to fill out and manage your Patient Information Authorization Form effortlessly. With user-friendly features such as editing, eSigning, and secure sharing, patients can manage their healthcare documents effectively. The platform ensures compliance with healthcare regulations, giving users peace of mind while handling sensitive documents.
How to fill out the patient information authorization form
-
1.To access the Patient Information Authorization Form on pdfFiller, visit the website and use the search bar to locate the form by its name.
-
2.Once discovered, click on the form link to open it directly in the pdfFiller interface.
-
3.Before starting to fill out the form, gather all necessary information including personal details, emergency contacts, and insurance information.
-
4.Begin completing the form by entering the required information into each blank field, such as your name and date of birth, using the fields provided.
-
5.Use the checkboxes to indicate your preferences, for instance, whether you speak English or any emergency contacts you wish to provide.
-
6.If you have insurance, be sure to include all relevant details in the insurance section, ensuring accuracy for processing.
-
7.Review each section carefully to ensure all information is accurate and complete.
-
8.After completing the form, double-check for any missing fields or unchecked boxes that are necessary for your submission.
-
9.Once satisfied with your entries, you can save the form as a PDF or download it for your records.
-
10.To submit the form, use any online submission options available in pdfFiller or print it out to send via traditional mail as needed.

What information is required to complete the Patient Information Authorization Form?
You need to provide personal details like your name and date of birth, emergency contact information, and insurance details, as well as sign to authorize treatment and HIPAA privacy practices.
Is there a deadline to submit the Patient Information Authorization Form?
While the form does not have a specific deadline, it should be completed and submitted prior to any medical appointments to ensure timely processing of your information.
How can I submit the Patient Information Authorization Form?
You can submit the completed form online via pdfFiller, or print it out to send it through mail. Check with Lexington Women’s Care for their preferred submission method.
Do I need to provide any supporting documents with this form?
While the main form only requires personal and insurance information, it's advisable to have your insurance card and identification handy in case additional verification is needed.
What are common mistakes to avoid when filling out this form?
Common mistakes include leaving blank fields, not signing the document, or submitting incorrect insurance information. Always review your form before submission.
How long does it take to process the Patient Information Authorization Form?
Processing times may vary, but typically the form is reviewed promptly to facilitate a smooth medical appointment. Contact Lexington Women’s Care for specific inquiries.
Is notarization required for the Patient Information Authorization Form?
No, notarization is not required for this form. Signing the form is sufficient to authorize the necessary disclosures and treatments.
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.