Get the free Alaska HIPAA Authorization template
Show details
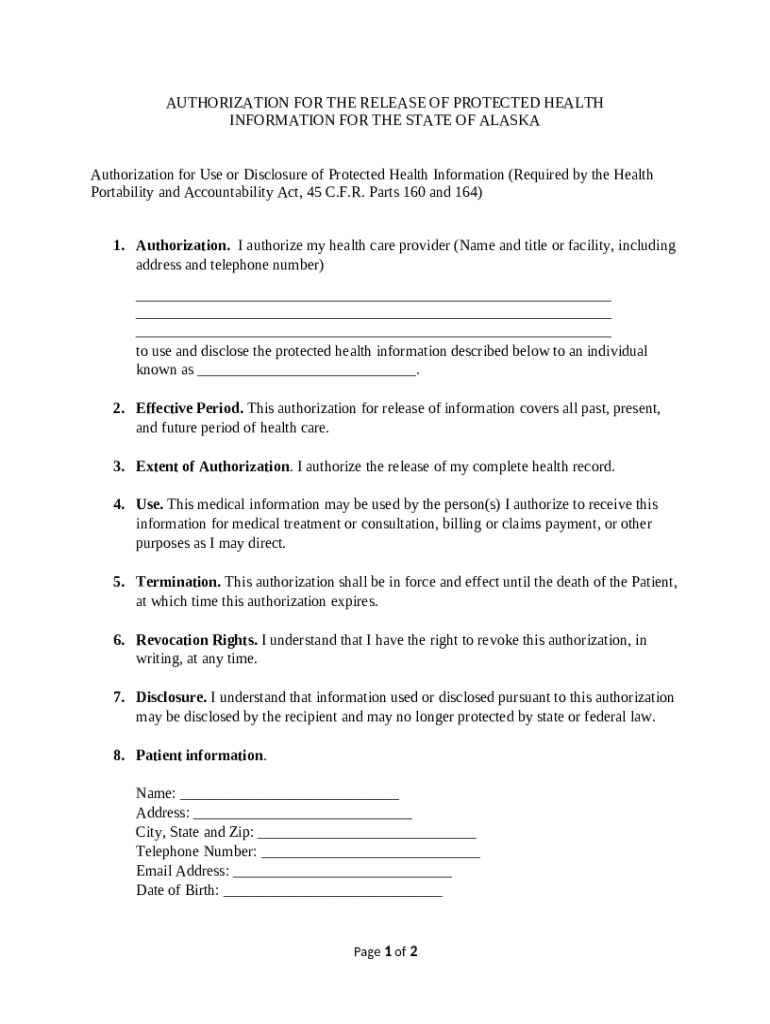
HIPAA authorization form specifically for Alaska
We are not affiliated with any brand or entity on this form
Fill out
Complete the form online in a simple drag-and-drop editor.
eSign
Add your legally binding signature or send the form for signing.
Share
Share the form via a link, letting anyone fill it out from any device.
Export
Download, print, email, or move the form to your cloud storage.
Why choose pdfFiller for your legal forms?
All-in-one solution
pdfFiller offers a PDF editor, eSignatures, file sharing, collaboration tools, and secure storage—all in one place.
Easy to use
pdfFiller is simple, cloud-based, has a mobile app, and requires no downloads or a steep learning curve.
Secure and compliant
With encryption, user authentication, and certifications like HIPAA, SOC 2 Type II, and PCI DSS, pdfFiller keeps sensitive legal forms secure.
What is alaska hipaa authorization
An Alaska HIPAA Authorization is a legal document that allows healthcare providers to disclose an individual's protected health information to third parties.
pdfFiller scores top ratings on review platforms
easy to use
easily add more files and combine them. easy to use
Easy
Very simple to use.I recommend it
astonished
i like this app but i am sencierly asking to one time option my ducuments are lock up so
great works well
great works well, easy to use
It is a great tool!
Great Product
Great Product. Easy to use
Who needs alaska hipaa authorization template?
Explore how professionals across industries use pdfFiller.

Alaska hipaa authorization template is needed by:
-
Individuals receiving medical treatment in Alaska
-
Healthcare providers in Alaska
-
Insurance companies requiring health information
-
Legal representatives of patients
-
Family members authorized to access health data
Alaska HIPAA Authorization Form Guide
How to fill out a Alaska HIPAA authorization form
Filling out an Alaska HIPAA authorization form is essential for allowing medical professionals to share your health information with third parties. To streamline this process, gather all pertinent health information and personal details before you begin. This guide will walk you through each aspect of the form.
Understanding HIPAA and authorization forms
The Health Insurance Portability and Accountability Act (HIPAA) is a federal law that protects your medical information from unauthorized disclosure. Authorization forms act as permissions, allowing healthcare providers to release your information under specific circumstances.
-
HIPAA creates standards for protecting sensitive patient information and ensures privacy during medical treatment.
-
An authorization form is a document that grants a healthcare provider the right to share your private health information.
-
Patient consent is critical as it safeguards individual privacy and controls how personal health details are handled.
Key components of the Alaska HIPAA authorization form
The Alaska HIPAA authorization form comprises several crucial sections that protect both provider and patient interests. Each component delineates the extent of information shared and the duration of consent.
-
This section requires the healthcare provider's information, including their full name, contact details, and address.
-
This specifies how long the authorization remains valid, ensuring that it cannot be interpreted as an indefinite consent.
-
This clarifies which specific medical records can be disclosed, protecting your privacy.
-
Outlines the purposes for which the recipient will utilize the shared information.
-
Indicates when and how the authorization can terminate, providing security to the individual.
-
Details your rights regarding when and how to withdraw the authorization after it has been granted.
-
This section elucidates potential risks associated with sharing personal information, ensuring you can make an informed decision.
How to fill out the Alaska HIPAA authorization form
Filling out the Alaska HIPAA authorization form correctly is crucial for ensuring compliance and safeguarding your rights. Here is a step-by-step guide to help you.
-
Carefully review the instructions for each form section, ensuring all fields are filled accurately.
-
Avoid leaving fields blank or providing incorrect information, as this may lead to delays in processing.
-
Use clear and concise language that specifies who can use the information and for what purpose.
Alaska-specific considerations for HIPAA compliance
Compliance with Alaska's specific HIPAA laws is essential when filling out the authorization form. Understanding local regulations can further ensure that you meet all legal requirements.
-
Alaska has state laws that enhance HIPAA protections, establishing additional privacy protections for residents.
-
State laws may provide more stringent guidelines for health information disclosure than federal regulations.
-
Consult with local legal resources to ensure all regulations are being appropriately followed.
Editing and managing your HIPAA authorization form with pdfFiller
pdfFiller offers a user-friendly platform to manage your Alaska HIPAA authorization form, allowing for seamless document management.
-
Simply upload your completed document and use the editing features to make any adjustments before finalizing.
-
Utilize the built-in eSignature tool to sign your document and securely share it with authorized recipients.
-
pdfFiller allows team collaboration, making it easier to manage health documents efficiently and securely.
Contact information for further queries
If you have additional questions regarding the authorization process, numerous resources and contacts are available.
-
Check the Alaska Department of Health website for comprehensive information and resources on HIPAA.
-
Reach out directly to state health department offices for specific inquiries about HIPAA compliance.
-
Contact pdfFiller support for help with any issues related to editing or managing your HIPAA authorization form.
How to fill out the alaska hipaa authorization template
-
1.Open the PDF version of the Alaska HIPAA Authorization on pdfFiller.
-
2.Begin by entering your personal information in the required fields, including your name, address, and date of birth.
-
3.Identify the person or entity to whom your health information will be disclosed by filling in their details.
-
4.Specify the types of health information that can be shared by marking the appropriate boxes.
-
5.Indicate the purpose of the disclosure, which can be for treatment, payment, or other reasons; select the option that applies to you.
-
6.Set the expiration date for the authorization, which is essential to limit how long your information can be shared.
-
7.Review the document for accuracy, ensuring all the information is correct and complete to avoid delays.
-
8.Sign and date the authorization at the designated area, confirming your consent to the disclosure of your health information.
-
9.Save the completed document and print copies for your records and for the designated recipient when necessary.
Related Pages
Related to alaska hipaa authorization template







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.