Get the free Authorization To Obtain Medical Treatment For Minor Child - Horse Equine s template
Show details
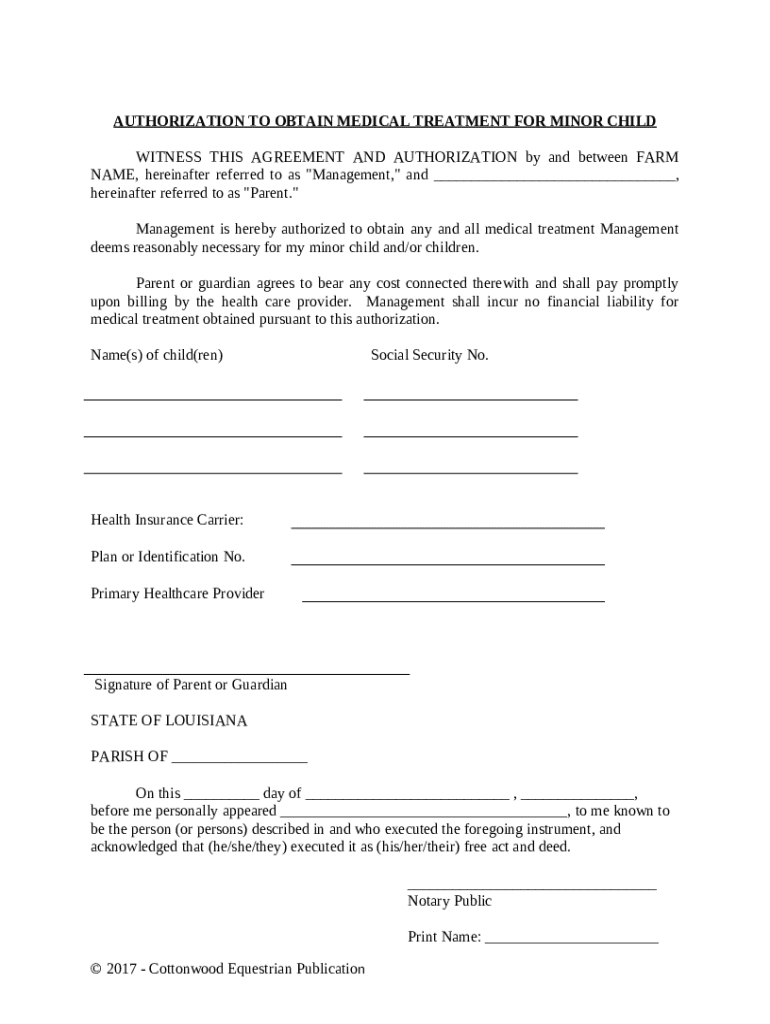
This Authorization To Obtain Medical Treatment For Minor Child. Horse Equine Form is an authorization form for medical treatment of a child that may be injured in connection with equine actvities.
We are not affiliated with any brand or entity on this form
Fill out
Complete the form online in a simple drag-and-drop editor.
eSign
Add your legally binding signature or send the form for signing.
Share
Share the form via a link, letting anyone fill it out from any device.
Export
Download, print, email, or move the form to your cloud storage.
Why choose pdfFiller for your legal forms?
All-in-one solution
pdfFiller offers a PDF editor, eSignatures, file sharing, collaboration tools, and secure storage—all in one place.
Easy to use
pdfFiller is simple, cloud-based, has a mobile app, and requires no downloads or a steep learning curve.
Secure and compliant
With encryption, user authentication, and certifications like HIPAA, SOC 2 Type II, and PCI DSS, pdfFiller keeps sensitive legal forms secure.
What is authorization to obtain medical
Authorization to obtain medical is a legal document that allows a designated individual or entity to access an individual's medical information.
pdfFiller scores top ratings on review platforms
this is awesome website, provides very helpful tools to edit any documents in any format.
Love this! Very easy, convenient and economical.
Great product without breaking the bank!
It is a great tool for business and personal use.
continues to provide a reliable method to modify and maintain our business model!
I hate how you cant Copy and past stuff from a word document or from similar sites back onto the PDFFILLER documents
Who needs authorization to obtain medical?
Explore how professionals across industries use pdfFiller.

Authorization to obtain medical is needed by:
-
Patients seeking to share their medical records with others.
-
Healthcare providers needing access to a patient's medical history for treatment.
-
Insurance companies requiring medical information to process claims.
-
Family members managing the healthcare of patients unable to provide consent themselves.
How to fill out the authorization to obtain medical
-
1.Download the authorization to obtain medical form from pdfFiller.
-
2.Open the form in pdfFiller's editor.
-
3.Fill in the patient's full name and date of birth in the designated fields.
-
4.Provide the name and contact information of the individual or organization authorized to receive the medical information.
-
5.Specify the type of medical information requested, such as records, test results, or treatment summaries.
-
6.Indicate the purpose of the information request, such as for personal records, insurance claims, or legal matters.
-
7.Include the date range for the requested medical records, if applicable.
-
8.Have the patient sign and date the form to indicate their consent.
-
9.Save the completed form and either print it for mailing or email it directly through pdfFiller to the appropriate party.
Related Pages
Related to authorization to obtain medical




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.