Last updated on Oct 22, 2015
Get the free Medicare Coverage Questionnaire Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
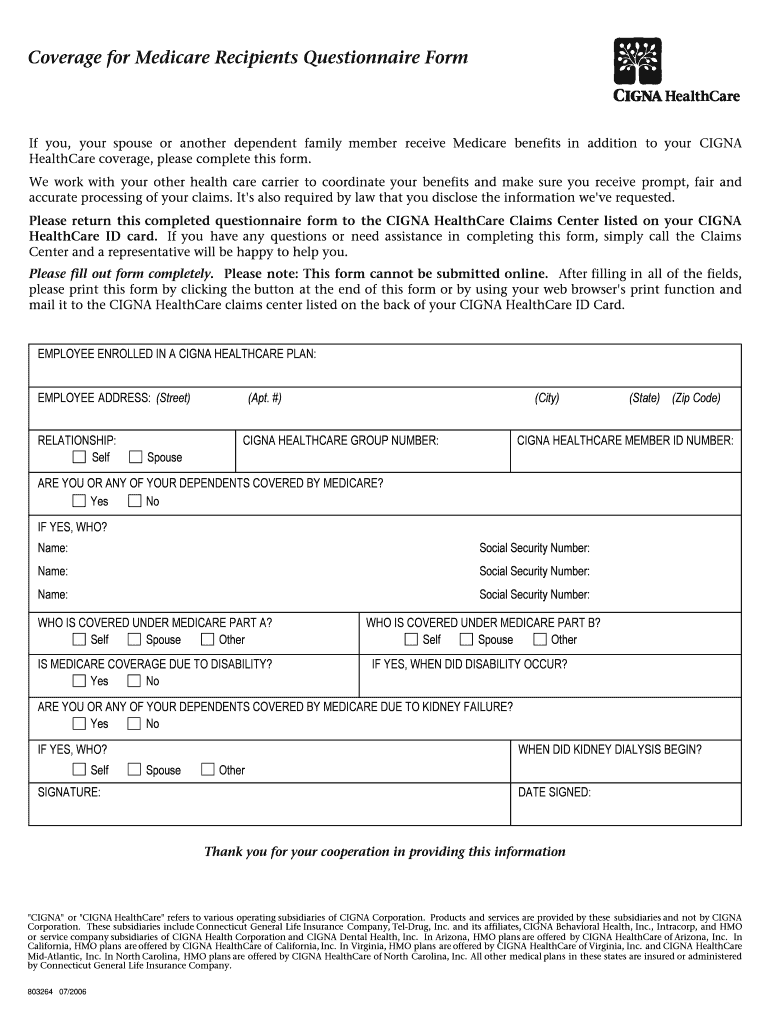
What is Medicare Questionnaire
The Medicare Coverage Questionnaire Form is a healthcare document used by CIGNA HealthCare to collect essential information from employees enrolled in their plans who also receive Medicare benefits.
pdfFiller scores top ratings on review platforms
Who needs Medicare Questionnaire?
Explore how professionals across industries use pdfFiller.

Medicare Questionnaire is needed by:
-
Employees enrolled in CIGNA HealthCare plans
-
Individuals receiving Medicare benefits
-
HR departments managing employee health coverage
-
Care coordinators assisting Medicare recipients
-
Insurance agents facilitating Medicare information
-
Healthcare providers verifying patient coverage
Comprehensive Guide to Medicare Questionnaire
What is the Medicare Coverage Questionnaire Form?
The Medicare Coverage Questionnaire Form is an essential tool utilized by CIGNA HealthCare to collect critical information regarding employees' Medicare benefits. This form serves a vital function in appropriately assessing Medicare coverage by gathering pertinent details from the employees enrolled in their healthcare plans.
By capturing essential data about individual Medicare benefits, this form aids in the accurate determination of coverage, which is crucial for both employees and CIGNA HealthCare. The information provided plays a key role in ensuring that employees receive the Medicare benefits that align with their specific needs.
Purpose and Benefits of the Medicare Coverage Questionnaire Form
The primary objective of the Medicare Coverage Questionnaire Form is to collect detailed information essential for evaluating Medicare coverage. This information facilitates a thorough understanding of each employee's healthcare needs and benefits.
Both CIGNA HealthCare and its employees stand to gain from the use of this form. For employees, it provides clarity on their Medicare coverage options, while CIGNA enhances its ability to determine coverage accuracy, thus optimizing healthcare delivery.
Who Needs to Complete the Medicare Coverage Questionnaire Form?
The target audience for the Medicare Coverage Questionnaire Form includes employees who are enrolled in CIGNA HealthCare plans and receive Medicare benefits. Specifically, anyone with Medicare Part A or B coverage needs to complete this form to ensure proper processing of their benefits.
Filling out this form is crucial for these individuals as it helps CIGNA HealthCare understand their coverage status, thereby enabling efficient service and support.
Key Features of the Medicare Coverage Questionnaire Form
The Medicare Coverage Questionnaire Form includes several key features that are important for accurate completion:
-
Required details such as employee address and relationship to the insured
-
Specific Medicare coverage status information
-
Multiple fillable fields to facilitate user input
-
Signature requirements to validate the form
-
Clear submission instructions for returning the completed form
These features collectively ensure that all necessary information is gathered efficiently, making the process smoother for both employees and CIGNA HealthCare.
How to Fill Out the Medicare Coverage Questionnaire Form Online (Step-by-Step)
Filling out the Medicare Coverage Questionnaire Form online can be streamlined by following these steps:
-
Access the online form through the designated platform.
-
Complete the 'EMPLOYEE ADDRESS' section accurately.
-
Provide necessary information in the 'RELATIONSHIP' field.
-
Enter your 'CIGNA HEALTHCARE MEMBER ID NUMBER' correctly.
-
Review all entries for accuracy before submitting.
By adhering to these steps, users can ensure thorough completion of the Medicare Coverage Questionnaire Form, promoting accurate processing of their benefits.
Common Errors and How to Avoid Them When Filing the Medicare Coverage Questionnaire Form
Customers frequently encounter a few common errors while completing the Medicare Coverage Questionnaire Form. Here are tips to avoid these pitfalls:
-
Double-check all personal information for accuracy, including name and address.
-
Ensure all required fields are filled completely to avoid delays.
-
Review the Medicare coverage details for correctness, especially for Part A and B coverage.
-
Include a signature and date where required.
Following a checklist can help in reviewing the completed form before submission, which can mitigate the likelihood of errors.
How to Submit the Medicare Coverage Questionnaire Form
Once the Medicare Coverage Questionnaire Form is completed, you have several submission options:
-
Print the form and mail it to the CIGNA HealthCare Claims Center.
-
Submit the form digitally, if available through your employee portal.
-
Use pdfFiller for online submission capabilities including eSigning and secure submission.
Understanding the timelines for processing and any documentation needed will support a smooth submission experience.
Security and Compliance for the Medicare Coverage Questionnaire Form
Ensuring data security is paramount when handling the Medicare Coverage Questionnaire Form. pdfFiller employs state-of-the-art security measures to protect sensitive information, including 256-bit encryption and compliance with HIPAA and GDPR regulations.
Utilizing secure sharing options as provided by pdfFiller further enhances privacy and ensures that users' data remains protected throughout the submission process.
What Happens After You Submit the Medicare Coverage Questionnaire Form?
Once the Medicare Coverage Questionnaire Form is submitted, CIGNA HealthCare undertakes several processing steps. Users can typically expect the following:
-
Initial review of submitted documents for completeness and accuracy.
-
A notification regarding the status of the application is usually provided.
-
Users can expect timely responses, keeping them informed of any follow-up needed.
Staying informed about the application status helps users manage their expectations regarding response times from CIGNA HealthCare.
Maximize Your Efficiency with pdfFiller to Complete Your Medicare Coverage Questionnaire Form
Using pdfFiller can significantly enhance the process of completing the Medicare Coverage Questionnaire Form. It offers features such as easy editing, eSigning capabilities, and secure submission options. This platform ensures that users have a smooth and efficient form-filling experience.
pdfFiller simplifies the entire procedure by streamlining steps that could be cumbersome through traditional means, making health care management easier for employees.
How to fill out the Medicare Questionnaire
-
1.Begin by accessing the Medicare Coverage Questionnaire Form on pdfFiller by searching for the form name in the platform’s search bar.
-
2.Open the form to reveal the fillable fields required for completion.
-
3.Before filling out the form, gather necessary information such as your address, relationship to the insured, and Medicare coverage details.
-
4.Use the fillable fields to input your EMPLOYEE ADDRESS accurately, specifying your RELATIONSHIP to the insured person.
-
5.Fill in the CIGNA HEALTHCARE GROUP NUMBER and CIGNA HEALTHCARE MEMBER ID NUMBER found on your insurance documents.
-
6.Next, provide your Medicare coverage status, indicating if you have Part A and Part B coverage.
-
7.Do not forget to address any disability-related Medicare coverage if applicable, including kidney failure-related details.
-
8.After completing all fields, review the information entered for accuracy by using pdfFiller’s review function.
-
9.Ensure you have filled out the form completely as instructed, and then locate the signature lines for your signature and date.
-
10.Once finalized, save your work by downloading the completed form in your preferred format or submit directly to CIGNA HealthCare Claims Center via pdfFiller’s submission options.

Who is eligible to use the Medicare Coverage Questionnaire Form?
Employees enrolled in CIGNA HealthCare plans who are also receiving Medicare benefits are eligible to use this form to provide necessary information.
What information do I need to complete the form?
To complete the Medicare Coverage Questionnaire Form, you will need your personal information, including your address, relationship to the insured, and Medicare coverage details, such as your Part A and Part B status.
How do I submit the completed form?
After filling out the Medicare Coverage Questionnaire Form, you can print it and mail it to the CIGNA HealthCare Claims Center. Alternatively, check if electronic submission is an option through pdfFiller.
Are there any supporting documents required when submitting the form?
Typically, supporting documents such as proof of Medicare coverage may not be required with this form, but it is advised to verify requirements directly with CIGNA HealthCare.
What are common mistakes to avoid when filling out the form?
Common mistakes include omitting required fields, incorrect relationship descriptions, and failing to sign the form. Double-check that all fields are filled accurately before submission.
What are the processing times for the form?
Processing times can vary, but generally, it may take several weeks for CIGNA HealthCare to process the form after receipt. Contact CIGNA for specific timing estimates.
Is notarization required for this form?
No, notarization is not required for the Medicare Coverage Questionnaire Form, making it easier to complete and submit through standard procedures.
Related Forms



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.