Last updated on Apr 10, 2026
Get the free Health Information Authorization Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
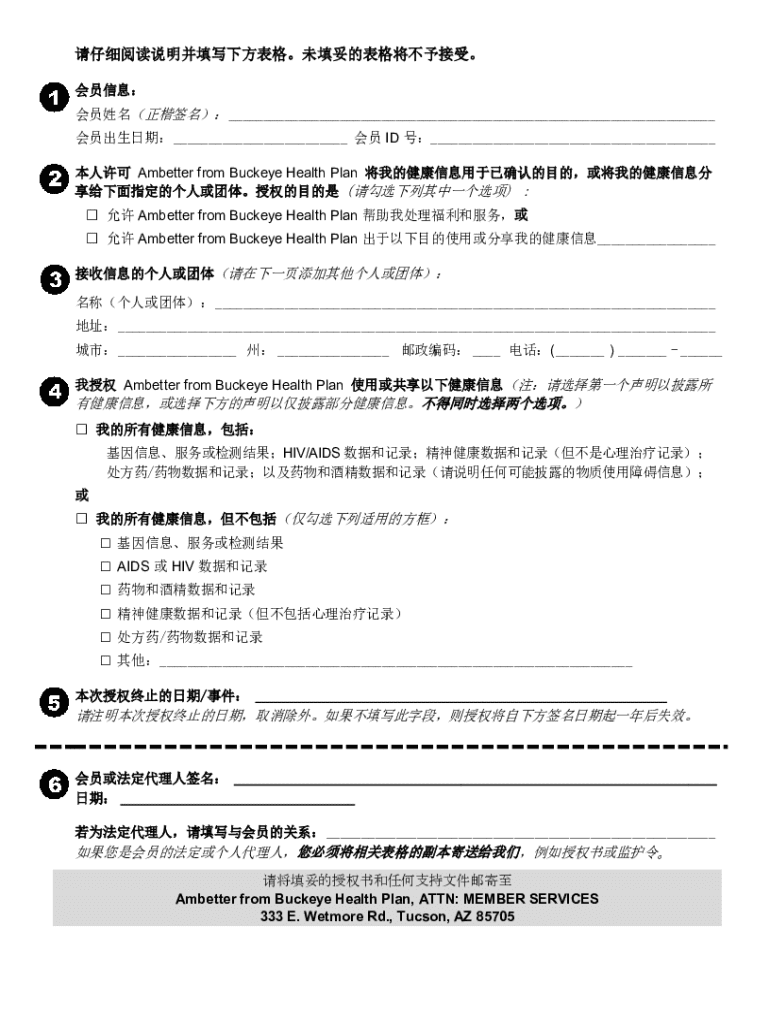
What is health information authorization form
The Health Information Authorization Form is a medical records release form used by members of Ambetter from Buckeye Health Plan to authorize the use and sharing of their health information.
pdfFiller scores top ratings on review platforms
Who needs health information authorization form?
Explore how professionals across industries use pdfFiller.

Health information authorization form is needed by:
-
Members of Ambetter from Buckeye Health Plan
-
Legal representatives handling patient affairs
-
Healthcare providers requesting patient information
-
Organizations needing patient consent for health data utilization
-
Individuals interested in medical record disclosures
Comprehensive Guide to health information authorization form
What is the Health Information Authorization Form?
The Health Information Authorization Form is a crucial document for members of Ambetter from Buckeye Health Plan, facilitating the sharing of personal health information. The purpose of this form is to ensure that members have control over their health data, allowing specified individuals or entities to access it for defined purposes, such as treatment and payment processes.
Members and Legal Representatives are the key roles relevant to this form. The legal representative may sign on behalf of the member, highlighting the importance of having trusted individuals involved in health information management. This level of involvement is essential to maintain transparency and ensure appropriate use of sensitive information.
Purpose and Benefits of the Health Information Authorization Form
This authorization form empowers members to govern the disclosure of their health information while enhancing their access to medical data. By utilizing this form, members can ensure that their personal information remains private with only designated individuals accessing their data.
Informed consent is paramount in medical settings, affirming that individuals are making knowledgeable decisions about their health information. The form serves as a tool for members, reinforcing their rights and enabling better management of their healthcare experiences.
Key Features of the Health Information Authorization Form
The Health Information Authorization Form includes several functionalities that make it user-friendly. Members can fill out various fields, selecting checkboxes for specific permissions regarding who may access their health information.
Additionally, the form provides options for revoking authorization, ensuring members can easily update their consent as circumstances change. This flexibility is crucial for maintaining control over one’s personal health information.
Who Needs the Health Information Authorization Form?
The Health Information Authorization Form is necessary for individuals who want to share their health information with healthcare providers or entities. Scenarios where this is particularly important include referrals to specialists, where timely access to medical history can enhance patient care.
Legal representatives may also need to fill out this form, representing the interests of members in situations where they are unable to do so themselves. Understanding these roles helps clarify who may be involved in the consent process.
How to Fill Out the Health Information Authorization Form Online (Step-by-Step)
-
Access the Health Information Authorization Form on pdfFiller.
-
Complete each fillable field with accurate information, ensuring clarity.
-
Select the individuals or entities that are permitted to access your health information.
-
Review all entries to confirm their accuracy before submission.
-
Follow any specific instructions related to your health information needs.
-
Submit the form using the available submission methods provided.
Common Errors and How to Avoid Them When Completing the Health Information Authorization Form
Users often encounter common mistakes while filling out the Health Information Authorization Form. These include leaving required fields unanswered or not selecting the necessary permissions.
To mitigate these errors, it’s helpful to utilize a checklist that includes:
-
Reviewing each section of the form for completeness.
-
Validating that all required fields are filled accurately.
-
Ensuring that checkboxes reflect permissions granted.
Submission Methods for the Health Information Authorization Form
Once completed, the Health Information Authorization Form can be submitted through various methods. Members can mail the form to the designated address or opt for electronic submission via secure online platforms.
It’s essential to be aware of the timeframes associated with processing submissions to ensure that your health information is shared promptly. Understanding these timelines can help manage expectations regarding responses.
Security and Compliance Measures When Using the Health Information Authorization Form
Security is a significant aspect of managing the Health Information Authorization Form. pdfFiller employs robust security measures, including 256-bit encryption, adhering to regulations such as HIPAA and GDPR to safeguard sensitive information.
By prioritizing data privacy and confidentiality, members can feel secure in the knowledge that their health information will be handled responsibly and in compliance with legal standards.
Unlocking the Power of pdfFiller for Your Health Information Authorization Form Needs
pdfFiller provides users with powerful tools for editing, eSigning, and securely managing the Health Information Authorization Form. The platform streamlines the form-filling process, allowing for an efficient experience.
With user-friendly features, members can leverage pdfFiller’s capabilities, ensuring that their health information is processed accurately and efficiently.
Get Started with Your Health Information Authorization Form Today!
Utilize pdfFiller to effectively fill out your Health Information Authorization Form. Experience the convenience of online editing and submission, allowing for seamless management of your health data.
Begin your journey today by accessing the form through pdfFiller’s platform, equipped to meet your healthcare needs.
How to fill out the health information authorization form
-
1.To access the Health Information Authorization Form on pdfFiller, visit the pdfFiller website and search for the form by its name.
-
2.Once you've located the form, click to open it in the pdfFiller editor, where you'll find various fillable fields designed for easy completion.
-
3.Before starting to fill out the form, gather necessary information such as the member's full name, date of birth, and the specific health information to be shared.
-
4.Navigate through the form, filling in each required field carefully. Use the interactive checkboxes to select relevant options regarding health information disclosure.
-
5.Once all fields are completed, review the form for accuracy, ensuring that all necessary information is included and that you've made the appropriate selections.
-
6.Finally, save your progress and download the completed form. You can also submit it directly through pdfFiller by following the platform's submission instructions.

Who is eligible to use the Health Information Authorization Form?
Members of Ambetter from Buckeye Health Plan and their legal representatives are eligible to use this form to authorize the disclosure of health information.
What should I do if I need to revoke authorization after submitting the form?
The form includes instructions for revoking authorization. You can follow those instructions to inform the involved parties when you wish to revoke access to your health information.
How can I submit the completed Health Information Authorization Form?
You can submit the form through pdfFiller by following their submission process, or you may print it out and mail it to the relevant healthcare provider or organization.
Are there any required supporting documents when submitting this form?
Generally, it's advisable to include identification or proof of relationship to the member when submitting the form, especially if you're a legal representative.
What common mistakes should I avoid when filling out the form?
Ensure all required fields are filled in completely and accurately. Double-check names, checkboxes, and dates to avoid common errors that could delay processing.
How long does it take to process the authorization once submitted?
Processing times may vary depending on the organization receiving the form, but it often takes a few business days to a couple of weeks to process health information disclosures.
Is notarization required for the Health Information Authorization Form?
Notarization is not required for this form; however, ensure that the signature provided is valid and corresponds with the member's official records.
Related Forms



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.