Last updated on Mar 30, 2026
Get the free Authorization for Use or Disclosure of Protected Health Information
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
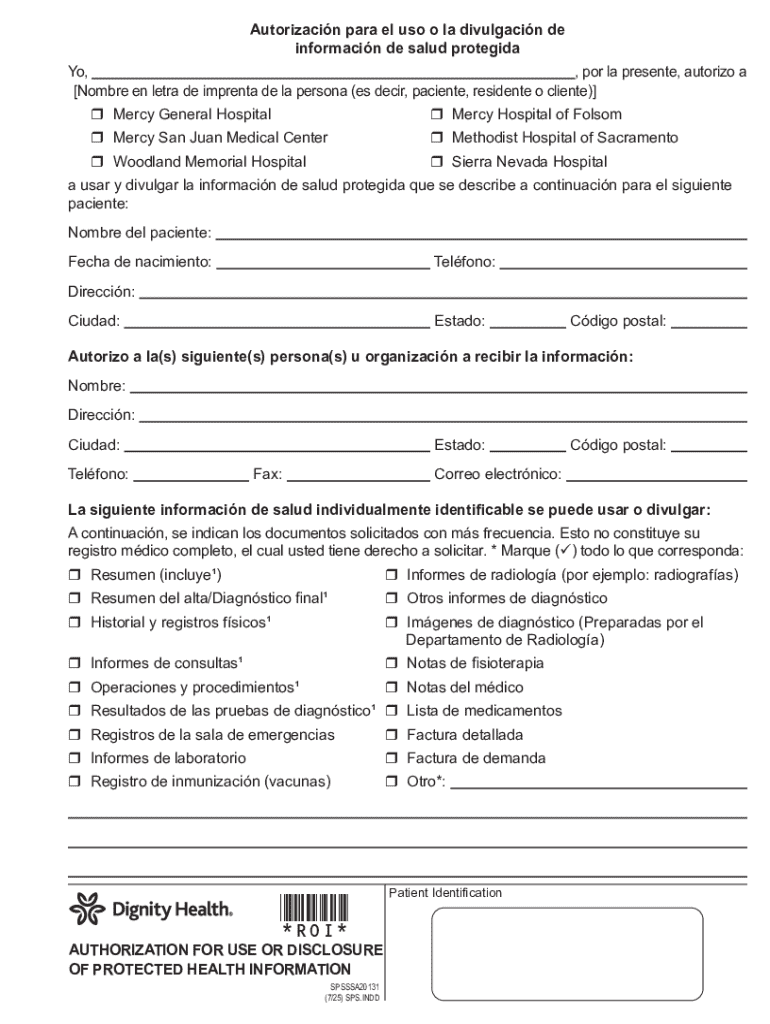
What is authorization for use or
The Authorization for Use or Disclosure of Protected Health Information is a healthcare form used by patients and personal representatives to permit the sharing of protected health information by healthcare providers in California.
pdfFiller scores top ratings on review platforms
Who needs authorization for use or?
Explore how professionals across industries use pdfFiller.

Authorization for use or is needed by:
-
Patients seeking to authorize medical information release
-
Personal representatives managing health information for others
-
Healthcare providers needing patient consent
-
Legal representatives for healthcare decisions
-
Hospitals requiring patient authorization
-
Insurance companies for health information access
Comprehensive Guide to authorization for use or
What is the Authorization for Use or Disclosure of Protected Health Information?
The Authorization for Use or Disclosure of Protected Health Information is a crucial document in healthcare, empowering patients to control who accesses their medical information. This health information authorization form is vital for fulfilling the primary goal of authorizing the use or disclosure of protected health information (PHI).
In California, medical consent plays an essential role, ensuring that patient preferences and rights are prioritized. Patients and their personal representatives are actively involved in the authorization process, guiding how their health information is shared among healthcare providers.
Purpose and Benefits of the Authorization for Use or Disclosure of Protected Health Information
This form is indispensable for both patients and healthcare providers, as it clarifies patient rights regarding their medical records. Patients can selectively authorize the release of their protected health information, enhancing confidentiality and trust in the healthcare system.
Having a structured process for the disclosure of health information ensures that patients' rights are upheld and promotes compliance with HIPAA regulations in California. Understanding the benefits of a well-drafted patient authorization template simplifies the administrative process while protecting patient privacy.
Who Needs the Authorization for Use or Disclosure of Protected Health Information?
Determining who requires this authorization is critical. A "patient" is defined as anyone receiving medical care, while a "personal representative" may act on the patient's behalf, particularly when they are unable to do so themselves.
Scenarios warranting the authorization include sharing medical records with family members or other healthcare providers, ensuring that all applicable individuals are included in the disclosure process. Understanding who needs a medical records release form helps maintain the integrity of health information management.
How to Fill Out the Authorization for Use or Disclosure of Protected Health Information (Step-by-Step)
Filling out the authorization form correctly is vital for effective communication of health information. Start by gathering essential information, including patient details and specific types of health information to be disclosed.
-
Enter patient information, including name and date of birth.
-
Select the specific types of information to be disclosed using checkboxes.
-
Fill in the recipient's information to whom the health information will be shared.
-
Sign and date the form, ensuring that a personal representative also signs where applicable.
Avoid common mistakes such as omitting required signatures or forgetting to specify the types of information being shared.
Key Features of the Authorization for Use or Disclosure of Protected Health Information
The authorization form is equipped with several essential fields. These include patient identification information, signature lines, and checkboxes for types of health information. Awareness of these features is crucial to ensure compliance and avoid issues.
-
Patient information fields such as name, address, and date of birth.
-
Signature lines for both the patient and personal representative.
-
Checkboxes for indicating the specific health information types being released.
-
Stipulations regarding the duration of the authorization’s validity.
-
Clear statements of the patient's rights related to their health information.
Security and Compliance for the Authorization for Use or Disclosure of Protected Health Information
Ensuring the security of sensitive health information is paramount when handling authorizations. Utilizing secure methods for transmitting the authorization is crucial to protect patient data.
pdfFiller adheres to rigorous security measures and complies with HIPAA standards, providing users with a safe platform for managing their health information. Taking precautions in the handling of the completed form can mitigate risks of unauthorized access.
How to Submit the Authorization for Use or Disclosure of Protected Health Information
Submitting the authorization form can be done through various methods. Patients can provide the form in person, send it by mail, or submit it electronically depending on the healthcare provider’s accepted practices.
-
In-person submission at the healthcare facility.
-
Mailing the completed form to the designated office.
-
Electronic submission through secure online portals.
-
Be aware of associated fees, if applicable, during submission.
-
Track and confirm the status of your submission for assurance.
What Happens After You Submit the Authorization for Use or Disclosure of Protected Health Information?
Once submitted, the authorization typically undergoes processing, which may vary in duration. Understanding the timeline for processing is essential for managing expectations.
Possible outcomes include approval or denial of the request to share health information, with specific reasons provided in case of denial. If delays occur, knowing how to follow up can facilitate resolution.
Sample or Example of a Completed Authorization for Use or Disclosure of Protected Health Information
Providing a visual or text-based example of a completed authorization form can help users better understand how to fill it out effectively. An annotated breakdown allows individuals to see what each section should look like when filled correctly.
Key tips for ensuring all necessary fields are filled out include double-checking personal information and confirming that all required signatures are present.
Empower Your Health Management with pdfFiller
pdfFiller offers robust functionalities for filling out, signing, and managing the authorization form, making it a convenient choice for users. Its security features ensure that your health information remains protected.
Explore additional document management capabilities offered by pdfFiller to streamline your healthcare processes and maintain control over your medical documents.
How to fill out the authorization for use or
-
1.To begin, access pdfFiller and search for the Authorization for Use or Disclosure of Protected Health Information form.
-
2.Once the form is opened, review the fields that need to be filled. You will see sections for patient details, types of health information, and recipient information.
-
3.Before filling out the form, gather necessary information, including your full name, contact information, and details of the health information to be released.
-
4.Use the text fields in pdfFiller to enter your personal details thoroughly.
-
5.Select the types of health information to be disclosed using the checkboxes provided in the form.
-
6.In the recipient information section, be sure to include the name and contact details of the entity or individual receiving the health information.
-
7.Once completed, review all the information entered to ensure accuracy and completeness.
-
8.After reviewing, finalize the form by adding your signature or that of your personal representative. pdfFiller allows you to sign electronically.
-
9.To save your work, use the ‘Save’ feature in pdfFiller. You can also download the form as a PDF or choose to submit it directly through the platform.

Who is eligible to use this authorization form?
This form is for patients or their personal representatives in California who wish to authorize the use or disclosure of their protected health information by healthcare providers.
Are there any deadlines for submitting this form?
There are no specific deadlines for submitting the Authorization for Use or Disclosure of Protected Health Information, but it should be completed and submitted before any healthcare service requiring information disclosure.
How can I submit the completed form?
You can submit this form by either downloading it and sending it to the healthcare provider or using electronic submission methods offered by some healthcare systems.
What supporting documents do I need to provide with this form?
Typically, you may need to provide proof of identity such as a government-issued ID, and additional documentation may be required if you are a personal representative acting on behalf of a patient.
What are common mistakes to avoid when filling out this form?
Common mistakes include forgetting to sign the form, not specifying the types of health information to be disclosed, and submitting the form without including necessary recipient information.
How long does it take to process this authorization?
Processing times can vary depending on the healthcare provider, but you can generally expect a response within a few days to a week after submission.
Is notarization required for this form?
No, notarization is not required for the Authorization for Use or Disclosure of Protected Health Information, making it easier to complete and submit.
Related Forms





Related Catalogs
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.