Last updated on Oct 22, 2015

Get the free Pharmacy Prior Authorization Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
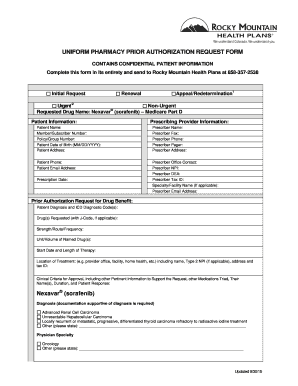
What is Prior Auth Form
The Pharmacy Prior Authorization Request Form is a healthcare document used by prescribers to request authorization for prescription drugs, especially Gazyva for chronic lymphocytic leukemia treatment.
pdfFiller scores top ratings on review platforms
Who needs Prior Auth Form?
Explore how professionals across industries use pdfFiller.

Prior Auth Form is needed by:
-
Oncologists submitting prior authorizations
-
Healthcare providers prescribing Gazyva
-
Patients needing chronic lymphocytic leukemia treatment
-
Insurance companies processing drug authorizations
-
Medical staff handling patient prescriptions
Comprehensive Guide to Prior Auth Form
What is the Pharmacy Prior Authorization Request Form?
The Pharmacy Prior Authorization Request Form is crucial for healthcare providers seeking prior authorization for prescription drugs. This form plays a significant role in ensuring that patients receive necessary medications, such as Gazyva (obinutuzumab), particularly for the treatment of chronic lymphocytic leukemia (CLL). By using the pharmacy prior authorization form, providers can facilitate the approval process for these essential treatments.
Purpose and Benefits of the Pharmacy Prior Authorization Request Form
This form is essential for both prescribers and patients. It not only benefits patients by expediting access to critical medications but also aids oncologists and healthcare providers in managing patient care effectively. The pharmacy prior auth template supports communication between prescribers and insurers, streamlining the approval process for vital treatments.
Key Features of the Pharmacy Prior Authorization Request Form
The Pharmacy Prior Authorization Request Form includes several key attributes essential for its effective use:
-
Patient name and identifying information
-
Prescriber details, such as name and contact information
-
Diagnosis details relevant to the treatment
-
Checkboxes indicating urgency of the request
-
Signature lines for prescriber authorization
Who Needs the Pharmacy Prior Authorization Request Form?
This form is primarily intended for oncologists and healthcare providers involved in the treatment of patients with CLL. It is crucial for ensuring that these providers can obtain necessary authorizations in a timely manner, ultimately supporting the patient's treatment journey. Understanding the importance of CLL treatment authorization helps streamline care processes.
How to Fill Out the Pharmacy Prior Authorization Request Form Online (Step-by-Step)
Completing the pharmacy prior authorization request form online is straightforward. Here are the step-by-step instructions:
-
Access the form online via the appropriate platform.
-
Fill in patient information, including names and identification details.
-
Enter prescriber information accurately, ensuring contact details are correct.
-
Provide a detailed diagnosis and any relevant medical history.
-
Select urgency by checking the appropriate box.
-
Ensure the prescriber reviews and signs the form before submission.
Submission Methods and Delivery
Once the Pharmacy Prior Authorization Request Form is completed, various submission methods are available:
-
Online submission through the designated healthcare platform
-
Mailing the form directly to the appropriate insurance provider
-
Faxing the completed form to expedite the process
Tracking the submission is essential to ensure timely handling and response from the insurance company.
Common Rejection Reasons and Solutions
Being aware of common rejection reasons can help users better prepare their submissions. The following are typical issues that may arise:
-
Incomplete patient or prescriber information
-
Missing diagnosis details or clinical criteria for approval
-
Failure to check urgency boxes appropriately
To avoid these issues, ensure all information is complete and accurate before submission. Validating details can significantly reduce the likelihood of rejection.
Security and Compliance for the Pharmacy Prior Authorization Request Form
Security is a top priority when handling sensitive healthcare documents. The Pharmacy Prior Authorization Request Form is constructed to comply with critical regulations, ensuring user data remains protected. pdfFiller employs various measures, including 256-bit encryption, to safeguard personal information and comply with HIPAA and GDPR guidelines, promoting privacy and data protection.
How pdfFiller Aids in Completing the Pharmacy Prior Authorization Request Form
pdfFiller significantly simplifies the process of completing the Pharmacy Prior Authorization Request Form. Its features include:
-
eSignature capabilities for secure approval
-
Fillable forms that enhance user experience
-
Accessible document sharing without the need for downloads
This makes the form-filling experience efficient and user-friendly across various devices.
Ready to Simplify Your Pharmacy Prior Authorization Process?
Utilizing pdfFiller for the Pharmacy Prior Authorization Request Form enhances convenience and efficiency. Engage with pdfFiller's robust platform to streamline your form processing and improve the overall authorization journey.
How to fill out the Prior Auth Form
-
1.To access the Pharmacy Prior Authorization Request Form on pdfFiller, go to the website and use the search bar to locate the specific form.
-
2.Open the form by clicking on it, which will launch the interactive interface where you can fill in the necessary information.
-
3.Before you begin, gather all required information such as patient details, diagnosis, and clinical criteria to ensure you complete all sections accurately.
-
4.Navigate through the form by clicking in each field to enter text. Use the checkboxes provided for urgent/non-urgent requests.
-
5.Fill in patient information including name and any relevant medical history. Be thorough and accurate in your entries.
-
6.Complete prescriber sections with your name, signature, and date to validate the request form.
-
7.Once all fields are filled, review the information for accuracy to avoid common errors and ensure all required data is provided.
-
8.Finalize the form by clicking the save button on pdfFiller, allowing you to keep a copy for your records.
-
9.To submit the form, use the submission options provided by pdfFiller, which may include email directly to Rocky Mountain Health Plans or download for mailing.

Who is eligible to fill out the Pharmacy Prior Authorization Request Form?
Any prescriber, particularly oncologists, who is requesting authorization for Gazyva prescriptions for their patients diagnosed with chronic lymphocytic leukemia is eligible to fill out this form.
What information do I need to complete the form?
You will need comprehensive patient information, prescriber details, diagnosis particulars, and clinical criteria for Gazyva treatment to complete the Pharmacy Prior Authorization Request Form accurately.
How do I submit the completed form?
Once you have completed the form on pdfFiller, you can submit it directly via email to Rocky Mountain Health Plans or download it for physical submission as per your preference.
What are common mistakes to avoid while filling the form?
Common mistakes include missing required fields, incorrect patient or prescriber information, and failing to sign the form. Ensure every detail is accurate and all sections are filled in before submission.
How long does the prior authorization process take?
The processing time for prior authorizations can vary based on the insurer but typically takes a few days. It's advisable to allow sufficient time for approvals before prescribing Gazyva.
Are there any fees associated with submitting the form?
Generally, there are no fees specifically for submitting a prior authorization request form. However, check with Rocky Mountain Health Plans for any potential costs associated with processing.
What happens if my prior authorization request is denied?
If a prior authorization request is denied, you can appeal the decision. Review the denial notice for reasons and conduct any necessary follow-up to provide additional information.
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.