Last updated on Oct 22, 2015
Get the free Pharmacy Prior Authorization Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
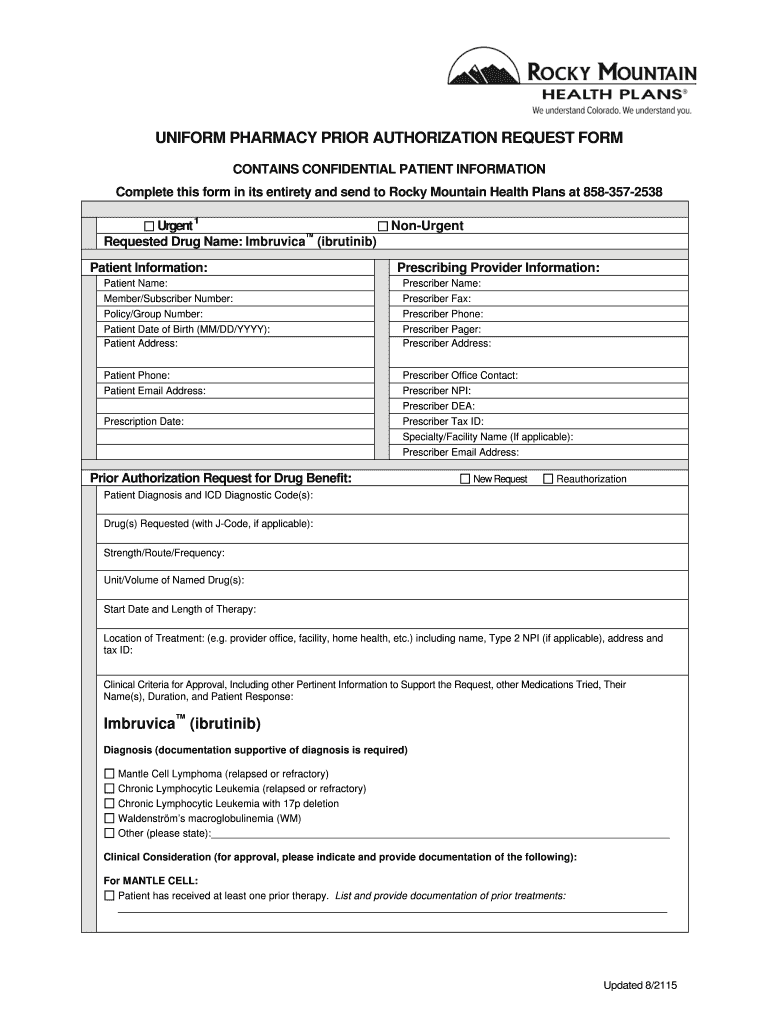
What is Prior Authorization Form
The Pharmacy Prior Authorization Request Form is a medical document used by healthcare providers to obtain prior authorization for medications like Imbruvica for patients requiring treatment.
pdfFiller scores top ratings on review platforms
Who needs Prior Authorization Form?
Explore how professionals across industries use pdfFiller.

Prior Authorization Form is needed by:
-
Healthcare Providers working with oncology patients
-
Prescribers needing medication approvals
-
Patients diagnosed with conditions like Mantle Cell Lymphoma
-
Pharmacists requiring authorization for prescriptions
-
Insurance agents handling healthcare plans
Comprehensive Guide to Prior Authorization Form
What is the Pharmacy Prior Authorization Request Form?
The Pharmacy Prior Authorization Request Form is a critical document used to seek approval for specific medications, such as Imbruvica, which is essential for treating conditions like Mantle Cell Lymphoma and Chronic Lymphocytic Leukemia. Healthcare providers such as doctors and nurses typically utilize this form to ensure that the necessary medications are covered by insurance before they are prescribed.
This authorization process is crucial as it allows for the effective management of patient treatment plans and helps avoid delays in medication access—for both prescribers and patients—by confirming coverage prior to dispensing the medication.
Purpose and Benefits of the Pharmacy Prior Authorization Request Form
The primary purpose of the Pharmacy Prior Authorization Request Form is to streamline the medication approval process for prescribers and patients alike. By efficiently managing treatment plans, the form plays a vital role in expediting approvals, which is particularly beneficial in urgent medical situations.
Notably, Rocky Mountain Health Plans is responsible for evaluating and approving these prior authorization requests, ensuring that patients receive the necessary medications promptly.
Key Features of the Pharmacy Prior Authorization Request Form
The Pharmacy Prior Authorization Request Form includes several essential fields to collect comprehensive information for processing. Information typically required on the form includes:
-
Patient information
-
Prescriber details
-
Clinical criteria related to the medication
-
Urgency checkboxes for immediate or standard requests
Additionally, the prescriber's signature is a necessary element, serving as an authentication step that validates the information provided.
Who Needs the Pharmacy Prior Authorization Request Form?
This form is primarily intended for healthcare providers, including physicians and pharmacists, as well as for patients who seek medications that require prior authorization. Certain medical conditions, such as Mantle Cell Lymphoma and Chronic Lymphocytic Leukemia, frequently necessitate the completion of this form to ensure coverage.
How to Fill Out the Pharmacy Prior Authorization Request Form Online
To efficiently complete the Pharmacy Prior Authorization Request Form online using pdfFiller, follow these steps:
-
Access the form through pdfFiller's platform.
-
Fill in required patient and prescriber information, ensuring accuracy.
-
Specify the clinical criteria and check urgency options, if applicable.
-
Review all entries before submitting the form for completeness.
Common mistakes, such as incomplete information or missing signatures, can easily be avoided by double-checking all sections before submission.
Submission and Processing of the Pharmacy Prior Authorization Request Form
Once the Pharmacy Prior Authorization Request Form is completed, it must be submitted to Rocky Mountain Health Plans. It is important to follow the specified submission process to avoid processing delays.
Typical processing times can vary, but timely submissions are crucial. Late filings might result in denied requests or additional paperwork, thereby impeding patients' access to necessary medications.
What Happens After You Submit the Pharmacy Prior Authorization Request Form?
After submission, Rocky Mountain Health Plans reviews the request. Applicants can track the status of their submissions online or through direct communication with their prescriber. Common reasons for rejection may include unclear clinical criteria or incomplete information, which can often be rectified through additional documentation or appeal processes.
If additional information is required, prescribers may need to renew or resubmit the request, leading to necessary follow-ups to ensure coverage is maintained.
Security and Compliance for the Pharmacy Prior Authorization Request Form
When handling the Pharmacy Prior Authorization Request Form, ensuring data security is paramount, especially when working with sensitive patient information. Compliance with regulations such as HIPAA and GDPR is strictly observed, highlighting pdfFiller's commitment to maintaining security throughout the document management process.
How pdfFiller Helps with the Pharmacy Prior Authorization Request Form
pdfFiller offers robust capabilities for users to edit, fill, and electronically sign the Pharmacy Prior Authorization Request Form without the need for downloads. With a focus on secure document management, users can efficiently handle forms, ensuring that sensitive information is protected while meeting necessary compliance standards.
Examples and Resources Related to the Pharmacy Prior Authorization Request Form
For further assistance, users can download a sample of a completed Pharmacy Prior Authorization Request Form for reference. This resource can be invaluable for understanding the completion process and ensuring accuracy in submissions. Additional links and resources for navigating prior authorization processes are also available to support healthcare providers.
How to fill out the Prior Authorization Form
-
1.To access the Pharmacy Prior Authorization Request Form on pdfFiller, visit the pdfFiller website and log in to your account. Use the search bar to locate the form by typing its name.
-
2.Once you find the form, click to open it in the pdfFiller editor. Familiarize yourself with the interface, including the toolbox for filling out fields.
-
3.Before starting to fill out the form, gather all the necessary information such as patient details, diagnosis, and medication specifics, along with any signatures required.
-
4.Begin filling out the form by entering the patient and prescriber information in the designated fields. Use the tab key for easier navigation between fields.
-
5.For the diagnosis and clinical criteria sections, ensure you provide detailed and accurate information, using any relevant checkboxes as required.
-
6.When you've completed all the required fields, review the entire form carefully for any errors or omissions.
-
7.Finalize the form by signing it where indicated. Ensure all signatures are obtained before submission.
-
8.To save your form, click the save icon, or choose to download a copy for your records. You can also submit the form directly through pdfFiller by selecting the appropriate submission method.

Who qualifies to use the Pharmacy Prior Authorization Request Form?
The form is intended for healthcare providers who prescribe medications for patients with specific medical conditions requiring authorization, such as cancer treatments.
Are there deadlines for submitting the Pharmacy Prior Authorization Request Form?
It is advisable to submit the form as soon as a medication is prescribed to avoid treatment delays. Each insurance provider may have specific timeframes for requests.
What methods can I use to submit the Pharmacy Prior Authorization Request Form?
The form can typically be submitted online through your healthcare provider's portal, directly to the insurance company via email, or by fax, depending on the protocols established by Rocky Mountain Health Plans.
What supporting documents are required with the Pharmacy Prior Authorization Request Form?
You may need to provide clinical notes, previous treatment records, and any relevant test results to support the request for authorization.
What are common mistakes to avoid when completing this form?
Common mistakes include missing required information, not obtaining necessary signatures, and failing to provide supporting documents, which may result in delays or denial of authorization.
How long does it typically take to process the Pharmacy Prior Authorization Request?
Processing times can vary, but generally, it takes a few days to two weeks. Check with Rocky Mountain Health Plans for specific timelines related to your request.
What should I do if my request for prior authorization is denied?
If denied, review the denial letter for detailed reasons, then consult with the prescribing provider to consider an appeal or alternative treatment options.
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.