Last updated on Feb 28, 2026
Get the free Chronic Pain Management Request Form
Show details
Patient Information First and last name (at birth) SexMFYearMonthDayBirth dateHealth insurance numberFile number (internal use)Address (No., St.)REQUEST FOR CONSULTATIONCHRONIC PAIN MANAGEMENTCity
We are not affiliated with any brand or entity on this form
Fill out
Complete the form online in a simple drag-and-drop editor.
eSign
Add your legally binding signature or send the form for signing.
Share
Share the form via a link, letting anyone fill it out from any device.
Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is chronic pain management request
The Chronic Pain Management Request Form is a medical document used by healthcare professionals to refer patients for chronic pain management services.
pdfFiller scores top ratings on review platforms
Who needs chronic pain management request?
Explore how professionals across industries use pdfFiller.

Chronic pain management request is needed by:
-
Referring physicians seeking to manage patient care.
-
Patients experiencing chronic pain requiring specialized assistance.
-
Healthcare providers in pain management clinics.
-
Medical record custodians needing patient information.
-
Insurance companies addressing claims related to pain treatment.
-
Healthcare professionals coordinating multidisciplinary care.
Comprehensive Guide to chronic pain management request
What is the Chronic Pain Management Request Form?
The Chronic Pain Management Request Form serves as a crucial tool for referring patients to chronic pain management services. It collects essential patient details and pain history, enabling healthcare professionals to effectively document chronic pain issues. An important aspect of the form is the requirement for the referring physician's signature, ensuring accountability and compliance in patient care.
Purpose and Benefits of the Chronic Pain Management Request Form
This form enhances patient care by facilitating thorough documentation of chronic pain assessments. Healthcare professionals benefit through streamlined referral processes that improve overall efficiency. Additionally, the form is designed to comply with healthcare standards, ensuring both quality patient care and adherence to legal requirements.
Who Needs the Chronic Pain Management Request Form?
The primary users of this form include referring physicians and other healthcare professionals involved in patient care. Scenarios necessitating the form include referring patients to pain management clinics and specialists for further evaluation and treatment.
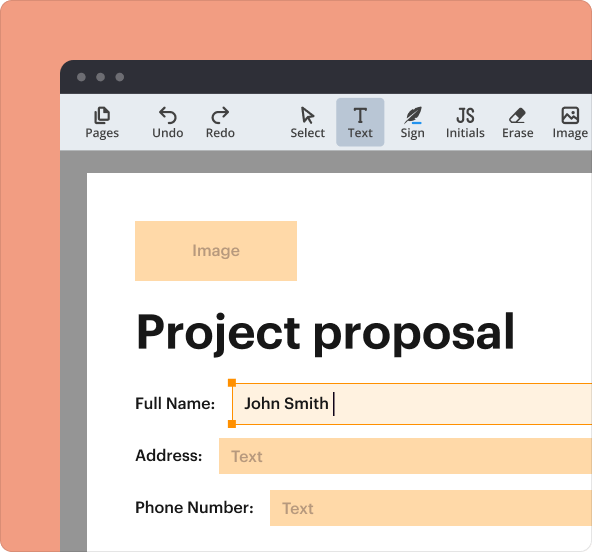
How to Fill Out the Chronic Pain Management Request Form Online (Step-by-Step)
Completing the form online is straightforward. Follow these steps for effective submission:
-
Enter personal details, including the patient's full name.
-
Provide accurate insurance information to facilitate coverage.
-
Detail the patient's pain history, including duration and intensity.
-
Review all information to ensure completeness and accuracy.
These steps help ensure that the information submitted is both accurate and comprehensive.
Field-by-Field Instructions for the Chronic Pain Management Request Form
Understanding each field of the form is crucial. Here’s a breakdown of essential fields:
-
First and last name: Clearly state the patient's name.
-
Health insurance number: Ensure this is up to date for billing purposes.
-
Address: Include full address details (number and street name).
-
Reason for request: Specify the reason for the pain management referral.
Be aware of common pitfalls in each section to avoid errors during submission.
What Happens After You Submit the Chronic Pain Management Request Form?
Upon submission, healthcare professionals can expect a confirmation of receipt. This process typically involves tracking the status of the referral and monitoring the patient's condition post-referral. Understanding what to expect helps maintain clear communication between patients and their healthcare providers during the referral period.
Security and Compliance for the Chronic Pain Management Request Form
Data security is paramount when handling the sensitive patient information required in the form. Compliance with privacy regulations such as HIPAA and GDPR is essential to protect patient data. pdfFiller is committed to ensuring document security, utilizing 256-bit encryption to safeguard information.
Common Errors and How to Avoid Them
Being aware of frequent mistakes made when filling out the form can significantly enhance accuracy. Consider the following best practices:
-
Double-check all entries for accuracy before submitting.
-
Use a checklist to ensure completion of each section.
These strategies help streamline the referral process and reduce the chances of errors.
How pdfFiller Can Help with the Chronic Pain Management Request Form
pdfFiller offers a cloud-based solution ideal for completing the Chronic Pain Management Request Form. Key features include editing capabilities, secure eSigning, and the ability to manage forms efficiently across the platform. Leveraging pdfFiller can simplify the form submission process, ensuring a smooth experience for both patients and healthcare professionals.
Sample of a Completed Chronic Pain Management Request Form
A visual example of a completed Chronic Pain Management Request Form can provide clarity on completing each section. Each part of the sample is annotated to assist healthcare professionals in understanding the necessary details for accurate form completion.
How to fill out the chronic pain management request
-
1.To access the Chronic Pain Management Request Form, visit pdfFiller and search for the specific title in the form library.
-
2.Once located, open the form by clicking on it which will launch it in the pdfFiller interface.
-
3.Before starting to fill out the form, gather all necessary patient information, including their full name, health insurance details, and previous pain management records.
-
4.Begin completing the form by entering personal details in the designated fields, utilizing pdfFiller's tools to navigate through the sections easily.
-
5.As you progress, provide the required insurance information and carefully note the patient's pain history and any previous interventions.
-
6.Be sure to check the checkbox for the reason for the referral; you can use the text box to elaborate if needed.
-
7.Review the entire form thoroughly for any missing or incorrect information, ensuring all sections are completed accurately.
-
8.Finalize the form by adding your signature in the designated area; ensure that your signature meets the required standards for submission.
-
9.Once completed, save your work within pdfFiller to ensure information is not lost.
-
10.You can download the filled form directly to your device or submit it electronically via the provided submission options in the pdfFiller interface.
Who is eligible to use the Chronic Pain Management Request Form?
The Chronic Pain Management Request Form is designed for healthcare professionals, most commonly referring physicians, who need to refer patients requiring chronic pain management services.
Are there deadlines for submitting the form?
While there are no specific deadlines stated, it is advisable to submit the form as soon as possible once the decision for referral is made to ensure timely access to pain management services.
How should I submit the completed form?
The completed Chronic Pain Management Request Form can be submitted electronically through pdfFiller or printed and mailed to the appropriate pain management clinic.
What supporting documents are needed with the form?
No specific supporting documents are outlined, but it is beneficial to include any relevant medical records, insurance information, and previous treatment history to support the referral.
What are some common mistakes to avoid when filling out the form?
Common mistakes include missing patient information, neglecting the signature, and not specifying the reason for the request. Careful review can help prevent these errors.
How long does it take to process this form?
Processing times will vary by clinic, but it typically ranges from a few days to a couple of weeks depending on the clinic's workload.
Is notarization required for this form?
No, the Chronic Pain Management Request Form does not require notarization, but it must be signed by the referring physician.
Related Forms

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.