Last updated on Mar 29, 2026
Get the free Direct Reimbursement Claim Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
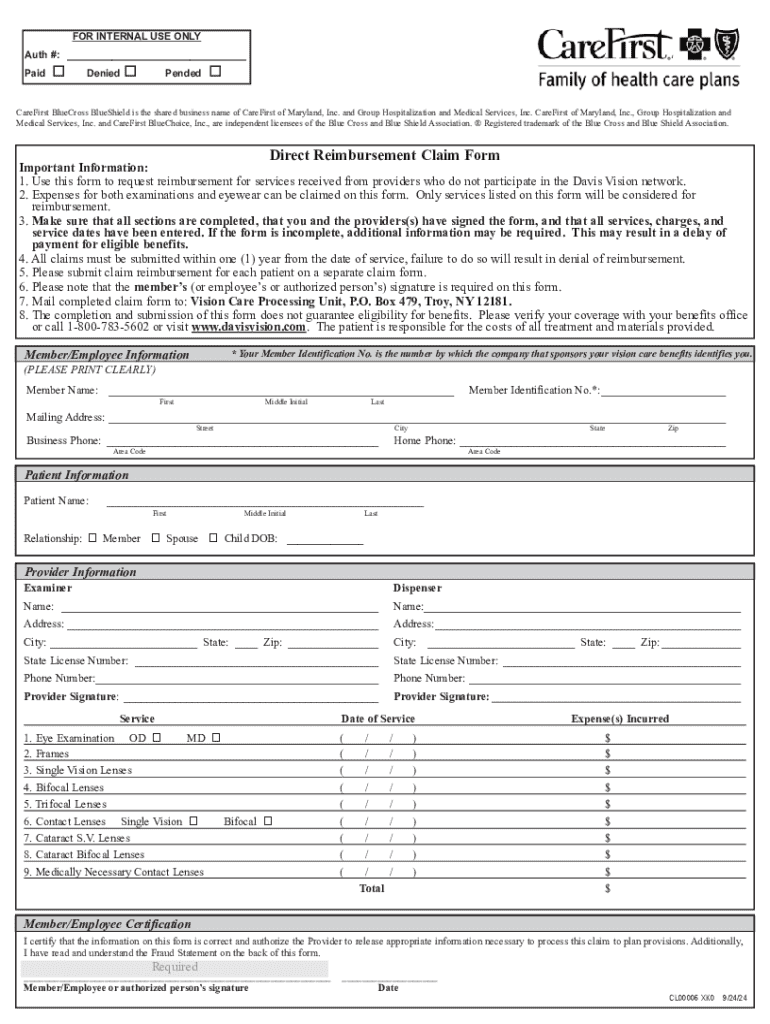
What is direct reimbursement claim form
The Direct Reimbursement Claim Form is a health insurance claim document used by members of the Davis Vision network to request reimbursement for services from non-participating providers.
pdfFiller scores top ratings on review platforms
Who needs direct reimbursement claim form?
Explore how professionals across industries use pdfFiller.

Direct reimbursement claim form is needed by:
-
Members of the Davis Vision network seeking reimbursement for vision services
-
Healthcare providers rendering services outside of the Davis Vision network
-
Insurance professionals handling reimbursement claims
-
Billing departments within healthcare facilities
-
Patients who have received vision care from non-participating providers
Comprehensive Guide to direct reimbursement claim form
What is the Direct Reimbursement Claim Form?
The Direct Reimbursement Claim Form is specifically designed for members of the Davis Vision network to request reimbursement for vision care services received from non-participating providers. This form plays a critical role in facilitating reimbursements for expenses related to examinations and eyewear. Members must be mindful of its time-sensitive nature; claims must be submitted within one year from the date of service.
Purpose and Benefits of the Direct Reimbursement Claim Form
The primary purpose of the Direct Reimbursement Claim Form is to streamline the reimbursement process for members. Utilizing this vision care reimbursement form accelerates access to funds and allows members to seek services from non-participating providers. By submitting this form, members can ensure they receive due compensation for their vision care expenses, enhancing their overall healthcare experience.
-
Facilitates quicker reimbursement processes.
-
Ensures access to services from non-participating providers.
-
Aids in receiving compensation for vision care costs.
Eligibility Criteria for Using the Direct Reimbursement Claim Form
To utilize the Direct Reimbursement Claim Form, both members and providers must complete the document. It is essential that signed consent is obtained from both parties involved. Certain exclusions exist, and there may be scenarios where the form is not applicable, such as for specific types of services or providers.
-
Members must complete the form for reimbursement requests.
-
Providers are required to provide necessary information and signatures.
-
Exclusions may apply based on service type or provider status.
How to Fill Out the Direct Reimbursement Claim Form Online (Step-by-Step)
Filling out the Direct Reimbursement Claim Form online involves several steps. Firstly, gather necessary preliminary information such as the member name, patient name, provider information, and date of service. Ensure that you complete each field accurately to avoid delays.
-
Enter the Member Name and Patient Name.
-
Provide accurate Provider Information.
-
Fill in the Service Date.
-
Review all entered details for accuracy.
-
Submit the form as per your preferred method.
Common Errors and How to Avoid Them
Common mistakes when completing the Direct Reimbursement Claim Form can lead to processing delays. To prevent these pitfalls, be aware of typical errors such as missing signatures or incorrect information. To assist you, here's a validation checklist to review before submission.
-
Check that all required fields are completed.
-
Ensure signatures from both member and provider are included.
-
Verify that the service date aligns with submission timeframes.
Submission Methods and What Happens After Submission
Members can submit the Direct Reimbursement Claim Form through various methods, including traditional mail or online submission. After submitting, expect confirmation of receipt and a processing time that typically varies based on submission method.
-
Submit via mail or online platforms.
-
Track your submission status after sending.
-
Processing times may vary; check the confirmation received.
Security and Compliance When Handling Your Claim Form
When transmitting personal and medical information, security is paramount. pdfFiller's platform adheres to stringent regulations such as HIPAA and GDPR, providing data protection measures including 256-bit encryption. Best practices for securely managing completed forms also apply, ensuring your information remains safe.
Leveraging pdfFiller for Your Direct Reimbursement Claim Form Needs
Using pdfFiller can significantly simplify the process of filling out and submitting your claim form. Key features include electronic signing, easy saving as a PDF, and access to a variety of form templates online. Explore how this cloud-based PDF management platform can enhance your experience through streamlined document management.
Sample or Example of a Completed Direct Reimbursement Claim Form
For users needing assistance, a visual or downloadable example of a completed Direct Reimbursement Claim Form is available. This sample illustrates what a properly filled out form looks like, clarifying each section's significance and expectations.
How to fill out the direct reimbursement claim form
-
1.Access pdfFiller and use the search function to locate the Direct Reimbursement Claim Form by entering its name.
-
2.Open the form and familiarize yourself with the fillable fields, which include sections for 'Member Name', 'Patient Name', 'Provider Information', and 'Service Date'.
-
3.Before filling out the form, gather necessary documents like receipts, service dates, and any previous correspondence related to your claim.
-
4.Begin filling out the form by clicking on each field and typing in the required information based on your gathered documents.
-
5.Ensure you complete all required fields, which may include checkboxes and signature lines indicated throughout the form.
-
6.After completing the form, carefully review all entered information for accuracy and completeness to avoid delays in processing.
-
7.Once you've confirmed that all information is correct, use the options in pdfFiller to save your filled form or download it for your records.
-
8.Submit the form by mailing it to the specified address for claims as outlined in the instructions that accompany the form.

Who is eligible to use the Direct Reimbursement Claim Form?
Eligibility for the Direct Reimbursement Claim Form includes any member of the Davis Vision network who has received vision services from a non-participating provider and is seeking reimbursement.
What is the deadline for submitting my claim?
Claims must be submitted within one year of the service date to be considered for reimbursement. Ensure your form is mailed before this deadline to avoid denial.
How do I submit the Direct Reimbursement Claim Form?
You must print the completed Direct Reimbursement Claim Form from pdfFiller, sign it, and mail it to the specified address for claims mentioned in the form instructions.
What supporting documents do I need to attach?
When submitting your claim, attach any receipts for services rendered, along with the completed claim form, to support your request for reimbursement.
What are common mistakes to avoid when filling out the form?
Common mistakes include skipping required fields, failing to provide signatures, and not attaching supporting documents. Double-check all entries before submission.
How long does it take to process my claim?
Processing times can vary, but typically claims are processed within several weeks. Keep track of your submission to ensure timely follow-up if delays occur.
What should I do if my claim is denied?
If your claim is denied, review the denial notice for reasons and consider contacting customer service for further clarification or to appeal the decision.
Related Forms



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.