Last updated on Mar 10, 2026
Get the free medicaid provider appeal request
Show details
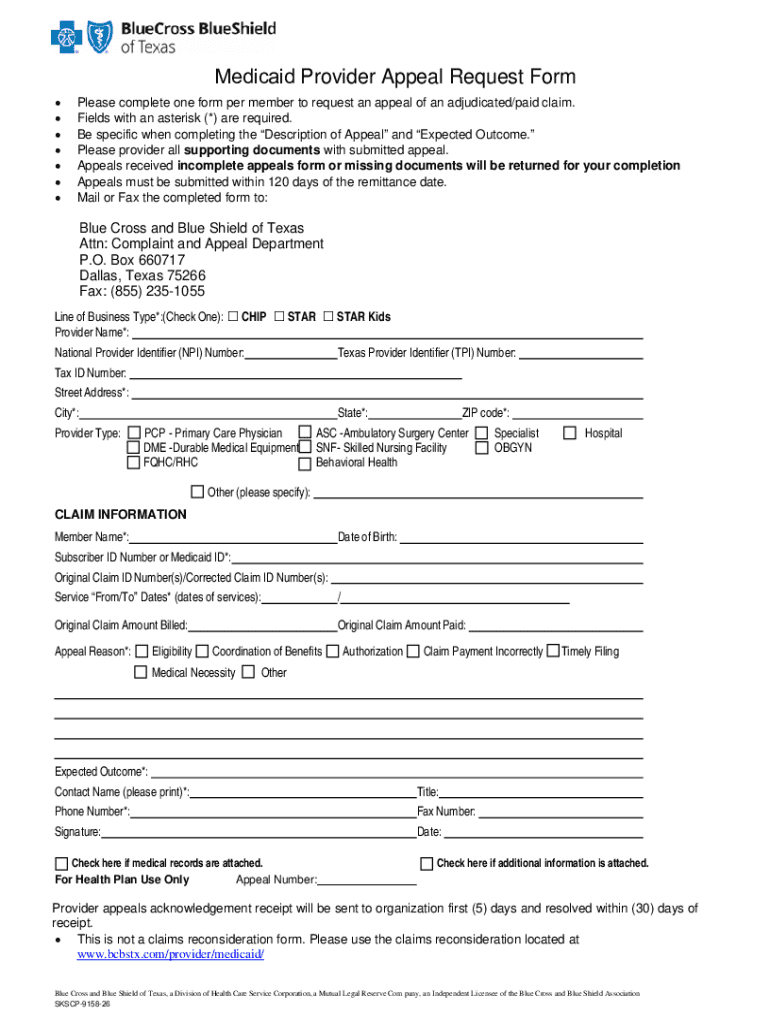
Medicaid Provider Appeal Request FormPlease complete one form per member to request an appeal of an adjudicated/paid claim. Fields with an asterisk (*) are required. Be specific when completing the
We are not affiliated with any brand or entity on this form
Fill out
Complete the form online in a simple drag-and-drop editor.
eSign
Add your legally binding signature or send the form for signing.
Share
Share the form via a link, letting anyone fill it out from any device.
Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is medicaid provider appeal request
The Medicaid Provider Appeal Request Form is a type of document used by healthcare providers in Texas to appeal an adjudicated or paid claim.
pdfFiller scores top ratings on review platforms
Who needs medicaid provider appeal request?
Explore how professionals across industries use pdfFiller.

Medicaid provider appeal request is needed by:
-
Healthcare providers in Texas
-
Medical billing specialists
-
Insurance claims processors
-
Healthcare administrators
-
Patient advocates
-
Legal representatives in healthcare
Comprehensive Guide to medicaid provider appeal request
What is the Medicaid Provider Appeal Request Form?
The Medicaid Provider Appeal Request Form is a crucial document utilized by healthcare providers in Texas for appealing adjudicated or paid claims. This form serves a significant role in the healthcare system, ensuring that providers can effectively contest decisions made by Medicaid regarding claim payments. Filling out this form accurately is essential, as it requires specific details to be provided, enhancing the chances of a successful appeal.
In Texas, this form is vital for maintaining the financial health of healthcare providers. By allowing for detailed disputes over claim decisions, the form empowers providers to advocate for their patients and secure necessary reimbursements. Accurate completion of the Medicaid Provider Appeal Request Form can greatly impact the efficacy of the appeals process.
Why Use the Medicaid Provider Appeal Request Form?
Utilizing the Medicaid Provider Appeal Request Form offers several benefits for healthcare providers. One primary advantage is the opportunity to appeal an already adjudicated or paid claim, which can lead to potential revenue recovery. By formally disputing adverse decisions, providers can reclaim funds that are rightfully theirs.
Additionally, using this form helps streamline the healthcare billing process. When appeals are correctly filed with all required information, it reduces the time spent on billing discrepancies and enhances overall operational efficiency.
Who Needs the Medicaid Provider Appeal Request Form?
The Medicaid Provider Appeal Request Form is designed for a wide range of healthcare providers in Texas. Eligible users include individual healthcare practitioners, medical groups, and healthcare institutions that bill Medicaid for services rendered. Understanding who can submit this form is crucial, as only authorized entities can contest Medicaid claims.
This form is specifically intended for those providers who wish to appeal claims made to Medicaid. Thus, in order to utilize the form effectively, it is essential for providers to ensure they meet all eligibility criteria.
Key Features of the Medicaid Provider Appeal Request Form
-
Fillable fields designed for easy data entry
-
Checkboxes to simplify selection and verification
-
Explicit instructions to guide users through the completion process
-
Required information about claims, healthcare providers, and members that must be included
-
Timelines specifying submission deadlines and acknowledgment periods
Each of these features is integral for ensuring that the form is filled out correctly, minimizing delays in the appeal process.
How to Fill Out the Medicaid Provider Appeal Request Form Online (Step-by-Step)
-
Gather all essential information, including claim details and provider data.
-
Access the Medicaid Provider Appeal Request Form online using a compatible web platform.
-
Complete the fillable fields accurately, adhering to any specific instructions provided.
-
Review the form carefully to avoid common errors before submission.
-
Submit the completed form via the desired method (online, mail, or in-person).
To ensure a smooth appeal process, be mindful of common pitfalls such as missing information or incorrect claim numbers, which can lead to processing delays.
Submission Methods and Deadlines for the Medicaid Provider Appeal Request Form
There are multiple options for submitting the Medicaid Provider Appeal Request Form. Providers can choose to send the form via mail, complete it online, or deliver it in-person to the relevant office. Each method has its own advantages, depending on the urgency of the appeal.
Providers should pay close attention to important deadlines. The form must be submitted within 120 days of the remittance date. Upon receipt, the submission will be acknowledged within five days, and a resolution is typically provided within thirty days.
What Happens After You Submit the Medicaid Provider Appeal Request Form?
After submitting the Medicaid Provider Appeal Request Form, healthcare providers can expect a thorough review and validation of their appeal. The status of the submission can usually be tracked through the appropriate channels, allowing providers to remain informed throughout the process.
In the event of a rejection, clear steps will be established to amend and resubmit the form. Understanding common rejection reasons can help in preparing a more robust appeal to improve chances of a favorable outcome in future attempts.
Security and Compliance for Your Medicaid Provider Appeal Request Form
Security is paramount when handling the Medicaid Provider Appeal Request Form. Providers must ensure that document handling practices comply with regulations such as HIPAA and GDPR. This compliance is crucial to protect sensitive patient information.
Using platforms such as pdfFiller provides additional security measures; the platform employs 256-bit encryption and follows SOC 2 Type II standards to safeguard data during the submission process. Prioritizing privacy and data protection is essential for maintaining trust in healthcare systems.
How pdfFiller Simplifies the Medicaid Provider Appeal Request Process
pdfFiller offers an array of tools designed to simplify the completion and submission of the Medicaid Provider Appeal Request Form. Key capabilities include editing, eSigning, and the ability to create fillable forms. These features enhance user experience by streamlining workflow.
Moreover, feedback from users highlights successful outcomes facilitated by pdfFiller's efficient document management system. This level of support is essential for healthcare providers navigating the complexities of appeals amidst busy operational environments.
Get Started with Your Medicaid Provider Appeal Request Today!
Utilize pdfFiller to ensure a seamless experience when completing the Medicaid Provider Appeal Request Form. The platform's intuitive features allow users to efficiently manage their appeals, leading to enhanced productivity and success rates.
With opportunities for new users to explore trial offers and specific features, engaging with pdfFiller will significantly streamline your appeals process in healthcare provided in Texas.
How to fill out the medicaid provider appeal request
-
1.Access the Medicaid Provider Appeal Request Form on pdfFiller by searching for the form name in the platform’s search bar.
-
2.Once the form opens, review the fillable fields and instructions provided on the document.
-
3.Gather all necessary information including claim details, provider information, member details, and any relevant supporting documents before you begin filling out the form.
-
4.Start completing the form by clicking into each fillable field and entering the required information. Utilize the checkboxes where applicable.
-
5.Make sure to follow the explicit instructions provided on the form to ensure that all sections are properly filled out.
-
6.After completing all fields, review the form for any errors or missing information. Ensure that all required documents are attached before submission.
-
7.Once you are satisfied with the form, save your progress to avoid losing any data. You can then download the completed form or submit it directly through pdfFiller.
Who is eligible to submit the Medicaid Provider Appeal Request Form?
Eligibility to submit this form is primarily for healthcare providers in Texas who need to appeal a paid or adjudicated claim.
What is the deadline for submitting the appeal request?
The completed Medicaid Provider Appeal Request Form must be submitted within 120 days from the remittance date of the claim.
How should the completed form be submitted?
The completed form can be submitted electronically through pdfFiller or printed and sent to the appropriate claims department as specified in the instructions.
What supporting documents are required with the appeal form?
You will need to attach any relevant documents that support your appeal, such as the original claim, remittance advice, or additional information regarding the claim.
What common mistakes should I avoid when filling out the form?
Ensure all fields are completed accurately, check for spelling errors, and confirm that you have included all necessary supporting documents to prevent delays in processing.
How long does it typically take to process an appeal?
The appeal will be acknowledged within 5 days, and a resolution is expected within 30 days of submission, barring any complications.
What should I do if my appeal is denied?
If your appeal is denied, review the denial notice for reasons provided and determine if further documentation can be submitted to support another appeal if warranted.
Related Forms


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.