Last updated on Mar 10, 2026
Get the free patient request form for
Show details
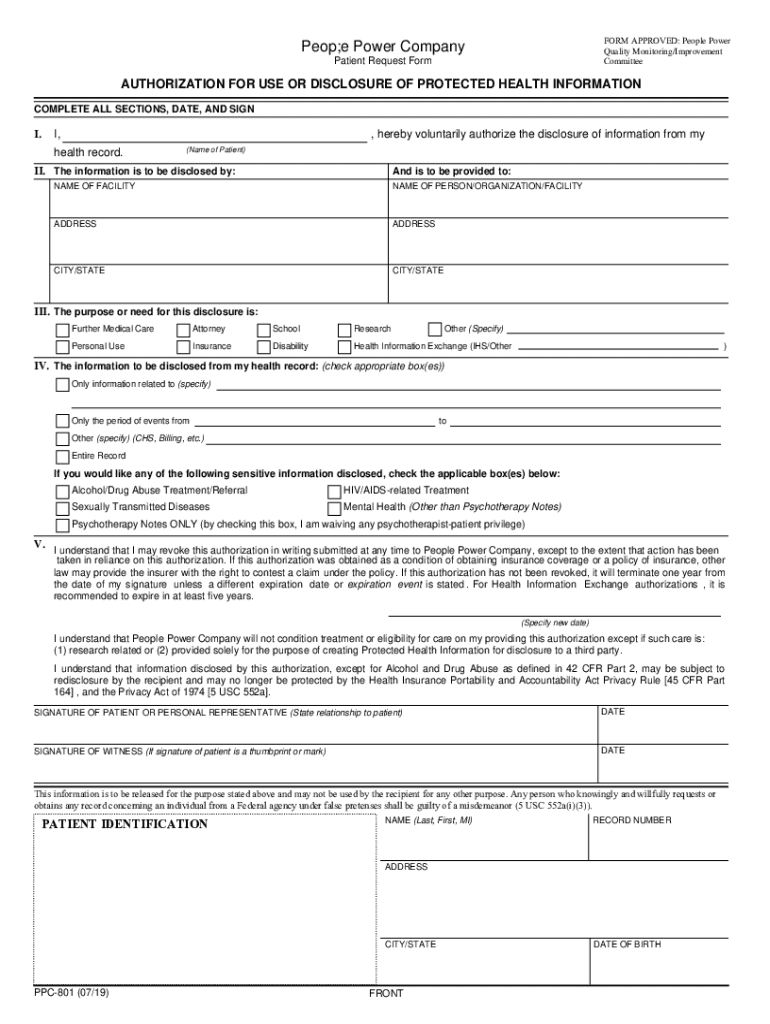
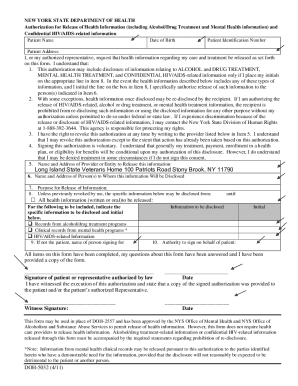
FORM APPROVED: People Power Quality Monitoring/Improvement CommitteePeop;e Power Company Patient Request FormAUTHORIZATION FOR USE OR DISCLOSURE OF PROTECTED HEALTH INFORMATION COMPLETE ALL SECTIONS,
We are not affiliated with any brand or entity on this form
Fill out
Complete the form online in a simple drag-and-drop editor.
eSign
Add your legally binding signature or send the form for signing.
Share
Share the form via a link, letting anyone fill it out from any device.
Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is patient request form for
The Patient Request Form for Health Information Disclosure is a legal document used by patients to authorize the release of their protected health information for specific purposes.
pdfFiller scores top ratings on review platforms
Who needs patient request form for?
Explore how professionals across industries use pdfFiller.

Patient request form for is needed by:
-
Patients seeking to access their health information
-
Healthcare providers needing patient consent for information sharing
-
Witnesses verifying the patient's signature when applicable
-
Medical facilities processing health record requests
-
Legal representatives helping patients with information retrieval
Comprehensive Guide to patient request form for
What is the Patient Request Form for Health Information Disclosure?
The Patient Request Form for Health Information Disclosure serves to facilitate the release of protected health information (PHI) by patients. Completing this form is crucial when requesting access to personal health data, ensuring compliance with privacy laws. This form not only specifies the information to be disclosed but also identifies the recipient and outlines the purpose of the request, offering a structured approach to health information disclosure.
Key aspects of PHI include any information that can identify an individual, including medical records, treatment history, and demographic details. By utilizing this patient request form, patients can effectively advocate for their rights while managing their healthcare information.
Why Do You Need the Patient Request Form for Health Information Disclosure?
Using the Patient Request Form provides numerous benefits, including legal protection and the promotion of privacy advocacy. This form ensures that patient authorization is obtained before any health information is shared, reinforcing the patient's control over their medical data.
Authorization through this form empowers patients in healthcare exchanges, as it validates their consent and outlines the parameters of information sharing. By taking proactive steps, patients can navigate their healthcare landscape more confidently.
Key Features of the Patient Request Form for Health Information Disclosure
The Patient Request Form includes several critical fields that must be completed accurately. These fields typically encompass:
-
Information to be disclosed
-
Recipient details, including name and contact information
-
Specific purpose for the request
Additionally, the form allows for options regarding the disclosure of sensitive information, ensuring patient preferences are respected. A signature is required from the patient, with a witness signature needed in certain instances, such as when the patient signs with a thumbprint or mark.
Who Should Use the Patient Request Form for Health Information Disclosure?
This form is primarily intended for patients who wish to manage their health information effectively. Moreover, a witness may be necessary to sign the form, especially in situations where the patient’s identity verification is required.
Specific scenarios warrant using this form, such as when patients are changing healthcare providers or need to share critical medical information with specialists. Understanding when and how to utilize this form is essential for patients seeking seamless healthcare management.
How to Complete the Patient Request Form for Health Information Disclosure (Step-by-Step)
Completing the Patient Request Form involves a series of straightforward steps:
-
Start by providing your personal identifying information, including name and contact details.
-
Specify the information to be disclosed and the intended recipient.
-
Clearly state the purpose of your request, ensuring that all options for sensitive information disclosure are noted.
-
Sign the form; if applicable, have a witness sign it as well.
To avoid common errors, review the form carefully after completion, ensuring that all necessary fields are filled and clear before submission.
Submission Methods for the Patient Request Form for Health Information Disclosure
The completed Patient Request Form can typically be submitted through various methods, including:
-
Email submission to the healthcare provider
-
Mailing the form via postal service
-
Delivering it in person to the provider's office
Be aware that there may be fees associated with processing this form, along with potential fee waivers for eligible individuals. After submission, processing times can vary, so it’s advisable to inquire about expected timelines with your healthcare provider.
What Happens After You Submit the Patient Request Form for Health Information Disclosure?
Upon submission, the healthcare provider will initiate the processing of your request. You can check the status of your request by contacting the provider’s office directly.
In the event of a rejection, patients have options for amendment, which may involve providing additional information or clarification to support their request. Understanding these steps can help manage expectations during the healthcare information exchange process.
Security and Compliance for the Patient Request Form for Health Information Disclosure
Security measures to protect sensitive information during this process are paramount. Utilizing platforms like pdfFiller incorporates robust encryption and compliance with standards such as HIPAA and GDPR to safeguard patient data.
Additionally, organizations are required to adhere to document retention policies and maintain privacy protections, ensuring that patient health information is handled with the utmost care and confidentiality.
Using pdfFiller for Your Patient Request Form for Health Information Disclosure
pdfFiller can significantly enhance the experience of completing and managing your Patient Request Form. The platform offers features like eSigning, fillable form options, and secure document storage, making the process straightforward and efficient.
Exploring pdfFiller can not only save time but also ensure accuracy in your form submissions, providing peace of mind while handling sensitive health information.
Sample Patient Request Form for Health Information Disclosure
For reference, a downloadable sample Patient Request Form is available. This example illustrates how to complete the form correctly, showcasing common fields and guidance on filling them in effectively.
Utilizing a sample can be especially helpful as you prepare your own request, ensuring all necessary components are included accurately to facilitate a seamless information disclosure process.
How to fill out the patient request form for
-
1.Access the Patient Request Form for Health Information Disclosure on pdfFiller. Search for the form in the pdfFiller search bar or navigate through the healthcare forms category.
-
2.Open the form to view all fields and sections. Familiarize yourself with the layout, noting where to input information.
-
3.Gather necessary information such as your personal details, the specific health information you wish to disclose, and the recipient's information before starting the form.
-
4.Begin filling in your name, address, and contact details in the designated fields. Ensure accuracy to avoid processing delays.
-
5.Specify the health information you want disclosed by checking the appropriate boxes or providing detailed descriptions in the relevant sections.
-
6.Indicate the purpose of the disclosure, which may involve selecting from predefined options or indicating a different reason in the form.
-
7.If required, arrange for a witness to sign the form alongside you. This is necessary if you are signing with a thumbprint or mark.
-
8.Review your completed form for accuracy, ensuring that all required fields are filled in and all necessary information is included.
-
9.Finalize the form by clicking the save option within pdfFiller. Check if you want to download it or submit it electronically through the platform.
-
10.Follow any prompts to finish submitting your request, making sure to retain a copy for your records.
Who is eligible to fill out the Patient Request Form for Health Information Disclosure?
Any patient in need of accessing their protected health information can fill out this form. Family members or legal representatives can also assist if they have been granted explicit authorization.
What are the submission methods for this form?
You can submit the completed Patient Request Form either electronically through pdfFiller or print and mail it to your healthcare provider. Ensure you follow the instructions provided by the recipient.
Are there any supporting documents required with the form?
Typically, no additional documents are required unless specified by your healthcare provider. However, include identification or any legal documents if requested, especially for legal representatives.
How long does it take to process the Patient Request Form?
Processing times can vary by provider, typically ranging from a few days to several weeks. It's best to confirm with the healthcare facility for their specific timeline.
What common mistakes should I avoid when filling out the form?
Ensure all fields are filled in completely and accurately, especially personal details. Double-check that you've signed the form in the required places and included a witness signature if necessary.
Is notarization required for this form?
No, notarization is not required for the Patient Request Form for Health Information Disclosure. However, ensure that you follow other specified requirements for valid signatures.
Can I save my progress while filling out this form?
Yes, pdfFiller allows you to save your progress as you fill out the Patient Request Form. This feature enables you to return to your form later if you need more time to complete it.
Related Forms
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.