Last updated on Mar 10, 2026
Get the free patient authorization form
Show details
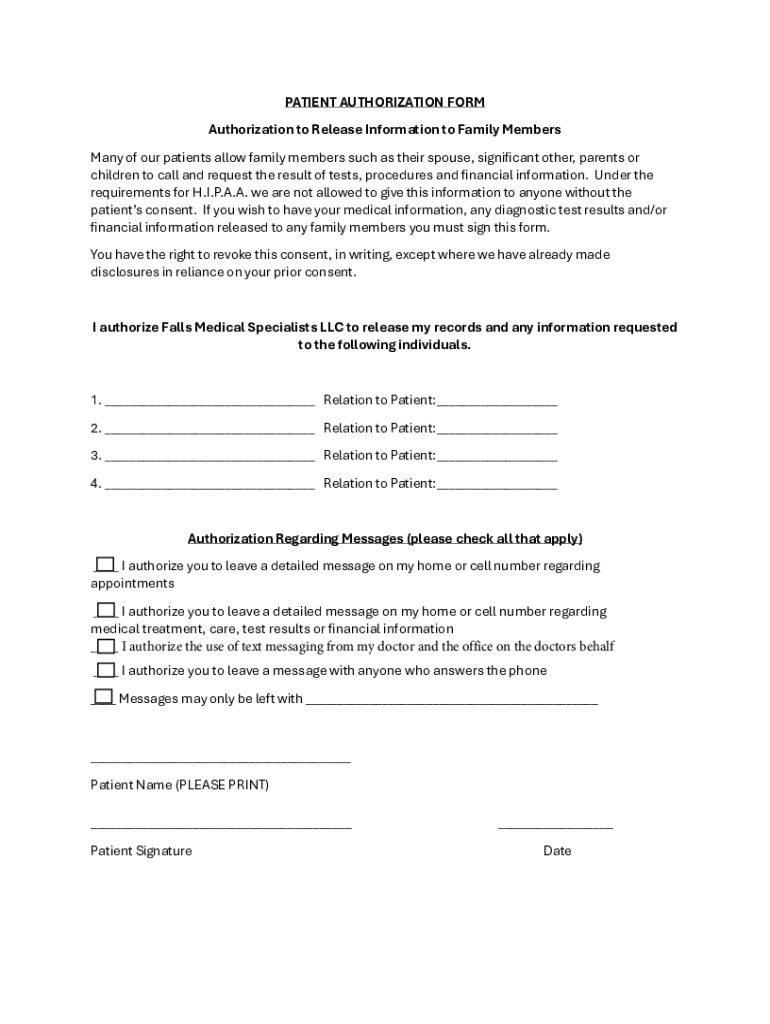
PATIENT AUTHORIZATION FORM Authorization to Release Information to Family Members Many of our patients allow family members such as their spouse, signicant other, parents or children to call and request
We are not affiliated with any brand or entity on this form
Fill out
Complete the form online in a simple drag-and-drop editor.
eSign
Add your legally binding signature or send the form for signing.
Share
Share the form via a link, letting anyone fill it out from any device.
Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is patient authorization form
The Patient Authorization Form is a healthcare document used by patients to grant permission to Falls Medical Specialists LLC to release their medical and financial information.
pdfFiller scores top ratings on review platforms
Who needs patient authorization form?
Explore how professionals across industries use pdfFiller.

Patient authorization form is needed by:
-
Patients seeking to authorize information release
-
Family members wanting access to medical details
-
Medical professionals needing patient consent
-
Healthcare administrators managing patient records
-
Legal representatives handling healthcare issues
Comprehensive Guide to patient authorization form
What is the Patient Authorization Form?
The Patient Authorization Form is a critical document enabling patients to grant permission to healthcare providers to release their medical information. This form is essential as it empowers patients by allowing them to control who has access to their medical records and under what circumstances it can be shared. By using a patient authorization form, individuals ensure their privacy is respected while navigating their healthcare journey.
Commonly referred to as a medical release form, this document must be accurately filled out to comply with legal and ethical standards in patient care.
Purpose and Benefits of the Patient Authorization Form
This form is vital for patients who need to authorize the release of their medical information to third parties such as family members or other healthcare providers. It creates a legal framework for sharing sensitive data while protecting the patient's rights.
Utilizing a patient consent form enables patients to actively participate in their healthcare decisions. The benefits include enhanced communication with healthcare professionals and family members and ensuring that personal health information is shared securely and only with authorized individuals.
Key Features of the Patient Authorization Form
The patient authorization form includes several key sections that capture essential information. Key areas consist of the patient's details, the relationships of individuals authorized to receive information, and specific authorizations regarding what information is shared.
Additionally, the form provides options for communication preferences related to treatments and finances, ensuring clarity and transparency.
Who Needs the Patient Authorization Form?
Patients and their family members are typically required to fill out this form when information needs to be shared. Scenarios warranting the form include when family members are involved in medical decision-making or finance-related discussions regarding treatment.
Healthcare providers may also use a patient authorization template to ensure compliance with legal requirements, particularly regarding HIPAA regulations.
How to Fill Out the Patient Authorization Form Online (Step-by-Step)
-
Access the Patient Authorization Form through pdfFiller’s online platform.
-
Enter your personal details in the designated fields, including your full name and contact information.
-
Specify the individuals authorized to receive your medical information.
-
Select the type of medical information to be shared and specify any limitations to the authorization.
-
Review the information entered for accuracy.
-
Sign the form digitally, ensuring that you comply with the necessary requirements.
-
Submit the completed form using the preferred method of delivery.
Common Errors and How to Avoid Them
When completing the Patient Authorization Form, common mistakes include failing to provide all necessary information or incorrectly signing the document. To avoid these errors, be thorough when filling out each section, and double-check the information provided before submission.
Ensuring the form is completely filled out and your signature matches the name listed is crucial for a valid submission.
Digital Signature vs. Wet Signature Requirements
Understanding the difference between digital signatures and traditional wet signatures is essential when submitting the Patient Authorization Form. Digital signatures offer a convenient and secure way to sign documents electronically, and they are recognized legally under HIPAA regulations.
This acceptance of electronic signatures facilitates the smooth processing of healthcare forms, promoting efficiency in sharing critical medical information while adhering to security protocols.
Submission Methods and Delivery of the Patient Authorization Form
The completed Patient Authorization Form can be submitted in several ways, including online via pdfFiller, mailing, or faxing the document. It is crucial to ensure that all sensitive information is handled securely during the submission process.
When opting for physical delivery, consider using secure mailing methods or verified fax lines to protect your personal data.
Security and Compliance for the Patient Authorization Form
Security measures for handling patient information are paramount when using platforms like pdfFiller. The system implements robust security protocols, including 256-bit encryption, to safeguard your data.
Moreover, pdfFiller complies with HIPAA and GDPR regulations, ensuring that your private information is treated with the utmost care and confidentiality.
Ready to Fill Out Your Patient Authorization Form?
Utilizing pdfFiller makes the process of completing your Patient Authorization Form easy and secure. With features such as eSigning and secure storage for your documents, you can efficiently manage your healthcare needs. Trust in pdfFiller’s established credibility and prioritize your healthcare information security.
How to fill out the patient authorization form
-
1.Start by accessing pdfFiller and searching for the Patient Authorization Form using the search bar.
-
2.Once located, click on the form to open it in the pdfFiller interface.
-
3.Familiarize yourself with the blank fields on the form, including sections for patient information, family relations, and authorization details.
-
4.Before starting, gather all necessary documents, such as identification and any information your family members need access to.
-
5.Begin filling out the form by clicking on the first field and entering your personal information, such as your name and contact details.
-
6.Continue navigating through the form, completing all required fields regarding who will be authorized to receive your medical information.
-
7.For each family member, provide their details accurately to avoid any processing delays.
-
8.Be sure to carefully read the options for authorizing messages regarding appointments and treatments before making your selections.
-
9.Once all fields are completed, take a moment to review the form thoroughly for accuracy.
-
10.Check that your signatures are included in the appropriate places, ensuring compliance with necessary requirements.
-
11.Use pdfFiller's 'Preview' option to see a final look at your form before saving.
-
12.To finalize, save the form by clicking the 'Save' button and choose your preferred format, such as PDF, for downloading.
-
13.If submitting directly from pdfFiller, follow the prompts to send the completed form to Falls Medical Specialists LLC.
What is the purpose of the Patient Authorization Form?
The Patient Authorization Form allows patients to authorize Falls Medical Specialists LLC to disclose their medical, diagnostic, and financial information to specified family members.
Who needs to fill out this form?
Patients who want to grant permission to family members or others to access their healthcare information must fill out this form.
Are there any deadlines for submitting the form?
While specific deadlines may vary, it's advisable to submit the Patient Authorization Form as soon as possible to avoid delays in accessing medical information.
Can I revoke my authorization once submitted?
Yes, patients can revoke their consent in writing at any time, and they should notify Falls Medical Specialists LLC about any changes.
What if I make a mistake while filling out the form?
If you make a mistake, use pdfFiller’s edit tools to correct it. Review your entries before finalizing to ensure all information is accurate.
How is the Patient Authorization Form submitted?
After completing the form on pdfFiller, you can submit it directly to Falls Medical Specialists LLC or download it and submit manually.
Is notarization required for this form?
The Patient Authorization Form does not require notarization, making it easier for patients to complete and submit.
Related Forms
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.