Last updated on Mar 14, 2026
Get the free patient referral form
Show details
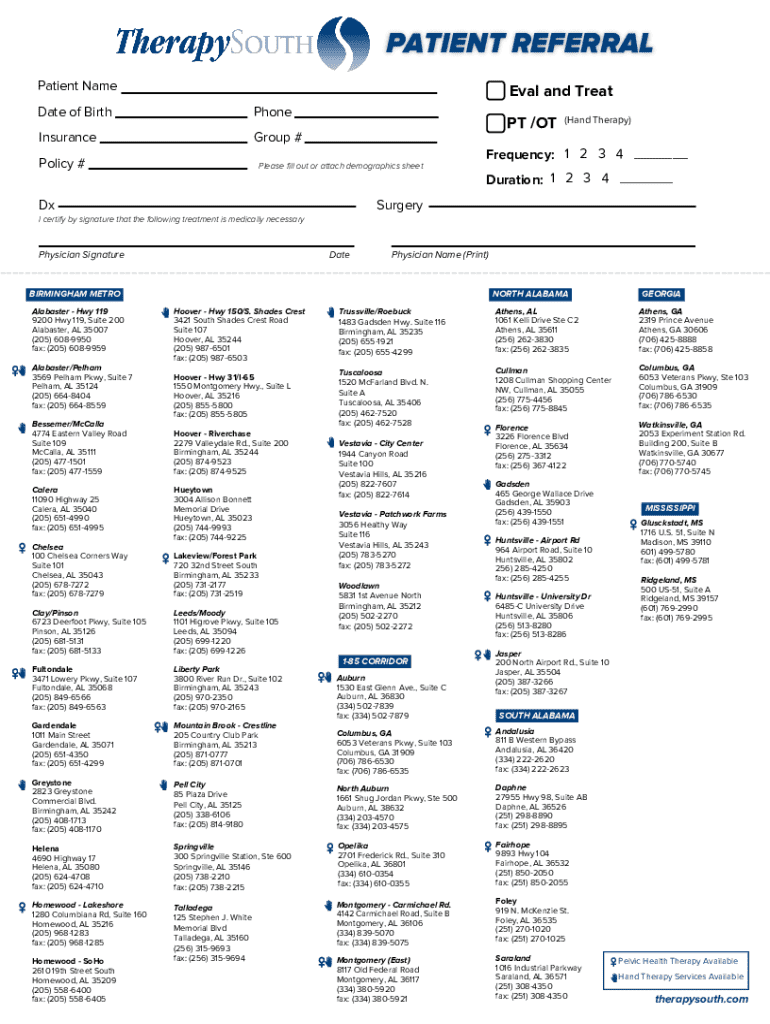
PATIENT REFERRAL Patient NameEval and TreatDate of BirthPhoneInsuranceGroup #Policy #Please fill out or attach demographics sheetPT /OT (Hand Therapy) Frequency: 1 2 3 4 ___ Duration: 1 2 3 4 ___DxSurgeryI
We are not affiliated with any brand or entity on this form
Fill out
Complete the form online in a simple drag-and-drop editor.
eSign
Add your legally binding signature or send the form for signing.
Share
Share the form via a link, letting anyone fill it out from any device.
Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is patient referral form
The Patient Referral Form is a healthcare document used by physicians to certify that treatment is medically necessary for patient referrals.
pdfFiller scores top ratings on review platforms
Who needs patient referral form?
Explore how professionals across industries use pdfFiller.

Patient referral form is needed by:
-
Physicians referring patients for treatment
-
Healthcare facilities handling patient admissions
-
Insurance companies reviewing referral requests
-
Patients seeking clarity on treatment necessity
-
Medical staff coordinating patient care
Comprehensive Guide to patient referral form
What is the Patient Referral Form?
The Patient Referral Form is a critical document in healthcare designed to certify that treatment is medically necessary. It facilitates the process of referring patients for evaluation and treatment by healthcare providers. This form plays a vital role in ensuring that patients receive the appropriate care they require.
Utilizing a medical referral form like this not only streamlines the referral process but also enhances the overall patient experience by clearly outlining treatment needs.
Purpose and Benefits of Using the Patient Referral Form
Employing the patient referral form offers numerous advantages for both patients and physicians. For healthcare providers, it simplifies the referral process, ensuring that essential information is relayed accurately. This efficiency translates directly to improved patient care and enhanced clarity regarding treatment needs.
The physician referral form ultimately promotes better communication between providers, leading to a more effective healthcare delivery system.
Key Features of the Patient Referral Form
This form includes important fields designed for seamless data entry and efficient processing of referrals. Key attributes of the form encompass:
-
Patient Name
-
Date of Birth
-
Insurance Group #
-
Check boxes for Frequency and Duration
-
A required signature line for the physician
The versatility of the medical necessity form makes it effective in capturing essential patient-related information accurately.
Who Needs to Use the Patient Referral Form?
The primary users of the patient referral form are healthcare providers, particularly physicians, who rely on this tool to enhance patient care. Patients must meet specific eligibility criteria to be referred, which can include medical conditions requiring specialist evaluation or treatments.
Instances that necessitate a referral may involve consultation with specialists or a need for specific therapeutic services, underscoring the form's role in the healthcare certification process.
How to Fill Out the Patient Referral Form Online (Step-by-Step)
Completing the Patient Referral Form correctly is crucial for ensuring accurate referrals. To help users navigate this process, here is a step-by-step guide:
-
Enter the patient's personal information, including the Patient Name and Date of Birth.
-
Provide contact information and insurance details, such as Insurance Group # and Policy #.
-
Select options for Frequency and Duration using the check boxes.
-
Ensure the form is signed by the physician in the designated signature line.
Attention to detail in each section will help prevent common mistakes and promote a successful referral.
Submission Methods and Next Steps After Completing the Patient Referral Form
Once the patient referral form has been completed, users can choose from several submission methods. Options include digital submission through healthcare platforms or physical delivery to the appropriate department.
After submitting the form, users can anticipate confirmation of receipt and a specified processing time, ensuring that the referral is processed promptly.
Security and Compliance When Using the Patient Referral Form
When handling sensitive patient information, security is paramount. The pdfFiller platform utilizes robust security measures, including 256-bit encryption, ensuring that all data is handled in accordance with HIPAA compliance.
To maintain data privacy while using the form, users are advised to follow best practices, which include securely storing documents and ensuring that only authorized personnel access sensitive information.
Sample of a Completed Patient Referral Form
To aid users in understanding how to accurately fill out the Patient Referral Form, a sample can be immensely valuable. This visual reference highlights the filled-out sections and demonstrates proper completion methods.
Users can download the sample form to explore its details before initiating their own referrals.
How pdfFiller Can Help You Fill Out the Patient Referral Form
pdfFiller offers a collection of tools designed to simplify the process of completing the Patient Referral Form. Users can easily edit, fill in, and electronically sign their forms using an efficient cloud-based platform.
Highlighted features include cloud access for documents, annotation capabilities, and straightforward sharing options that enhance collaboration among healthcare providers.
Take Your First Step Towards Efficient Referrals
By utilizing pdfFiller for your form needs, you can significantly streamline the referral process. The platform is designed for ease of access and saves time, ultimately enhancing the accuracy and security of your documentation.
Prioritizing correct and secure documentation is essential for maintaining the integrity of patient care.
How to fill out the patient referral form
-
1.To access the Patient Referral Form on pdfFiller, visit the website and search for 'Patient Referral Form' in the search bar.
-
2.Once the form is visible, click to open it. You will see the interactive fields where you can enter information.
-
3.Before filling out the form, gather necessary patient details such as the patient's name, date of birth, insurance information, and contact number.
-
4.Begin by entering the patient's name and date of birth in the designated fields. Ensure accuracy for reference.
-
5.Next, fill in the insurance details including the insurance group number and policy number for comprehensive information.
-
6.For information regarding treatment frequency and duration, utilize the checkboxes provided to specify the requirements.
-
7.After you have completed the fillable fields, review your entries to ensure all information is correct and complete.
-
8.Make sure to sign the form where indicated as physician certification is crucial to validate the referral.
-
9.Once you are satisfied with the information, save the form by clicking the 'Save' button, which allows you to keep a copy.
-
10.To download or submit the form, utilize the options available on pdfFiller to either print it out or send it directly to the necessary parties.
Who is eligible to use the Patient Referral Form?
The Patient Referral Form is primarily intended for physicians who need to refer patients for treatment, as well as healthcare facilities that process these referrals.
Are there any deadlines for submitting the Patient Referral Form?
While there are typically no strict deadlines for this form, it is advisable to submit it as soon as the treatment necessity is established to expedite patient care.
How should the Patient Referral Form be submitted?
The Patient Referral Form can be submitted digitally by using pdfFiller to send it directly to the appropriate healthcare provider or printed for manual submission.
What supporting documents are required when submitting this form?
Generally, you may need to attach patient medical records or insurance information that demonstrates the medical necessity of the referral along with the form.
What common mistakes should I avoid when filling out the form?
Ensure all fields are filled out completely and accurately, especially patient identification and insurance details, to avoid delays in processing the referral.
How long does it take to process a Patient Referral Form?
Processing times can vary by healthcare provider, but it usually takes a few business days to review and act upon the submitted referral.
Can I amend the Patient Referral Form after submission?
If you need to make changes after submission, contact the receiving healthcare facility directly to request the required updates or provide additional information.
Related Forms

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.