Last updated on Apr 10, 2026
Get the free Medication Authorization Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is medication authorization request form
The Medication Authorization Request Form is a healthcare document used by physicians to obtain insurance coverage for specific drugs like Tysabri.
pdfFiller scores top ratings on review platforms
Who needs medication authorization request form?
Explore how professionals across industries use pdfFiller.

Medication authorization request form is needed by:
-
Physicians managing patient drug therapies
-
Healthcare administrators in Michigan
-
Patients requiring medication approval
-
Insurance providers like Blue Cross Blue Shield of Michigan
-
Pharmacy staff processing medication requests
Comprehensive Guide to medication authorization request form
What is the Medication Authorization Request Form?
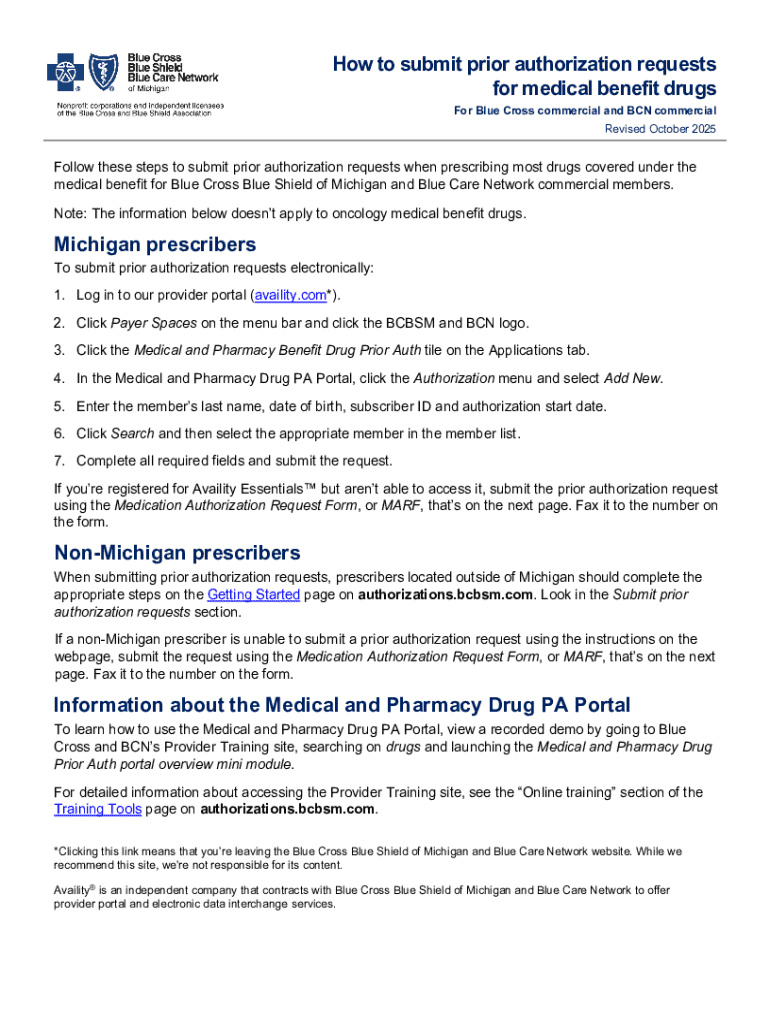
The Medication Authorization Request Form (MARF) is a crucial document that enables physicians to request coverage for specific medications from insurance providers. This form is particularly vital for obtaining coverage for drugs such as Tysabri and other medical benefit drugs, ensuring that patients have access to necessary treatments. It streamlines the process of acquiring drug coverage, making it an essential element in patient care.
Purpose and Benefits of the Medication Authorization Request Form
The primary purpose of the Medication Authorization Request Form is to facilitate the authorization process for healthcare providers. By utilizing this form, physicians can effectively secure authorization for specific medications necessary for treating their patients. This simplifies the workflow for physicians and enhances patient outcomes by improving access to essential treatments through a streamlined submission process.
Benefits of using the MARF include:
-
Efficient processing of drug requests
-
Reduced processing time for approvals
-
Enhanced access to medical benefit drugs for patients
Key Features of the Medication Authorization Request Form
The Medication Authorization Request Form includes several important features designed to assist both physicians and healthcare organizations. Essential fields within the form collect vital information such as:
-
Patient name and ID number
-
Diagnosis details
-
Physician information and signature
Additionally, users have options for submitting the form through various methods, including fax and an online portal, ensuring accessibility and convenience.
Who Needs the Medication Authorization Request Form?
This form is specifically designed for physicians who treat patients requiring authorization for drugs covered under their medical plans. It serves a wide range of patients, including those dealing with chronic conditions or specialized treatment needs. Physicians are encouraged to utilize the Medication Authorization Request Form for any medication requiring prior authorization.
How to Fill Out the Medication Authorization Request Form Online
Filling out the Medication Authorization Request Form online involves several critical steps to ensure accuracy and completeness. Follow this guide to complete the form effectively:
-
Enter the patient’s name and ID number in the designated fields.
-
Provide detailed diagnosis information accurately.
-
Ensure the physician’s signature is included at the required section.
Common pitfalls to avoid include missing checkboxes or incorrect patient details, which can delay processing and lead to potential rejections.
Submission Methods for the Medication Authorization Request Form
Submitting the Medication Authorization Request Form can be done through various methods. Physicians can choose to submit the form online or via fax. To ensure proper handling:
-
Check the accuracy of all entries prior to submission.
-
Confirm receipt of the form through the chosen submission method.
Best practices involve keeping copies of submitted forms and any confirmation received for future reference.
What Happens After You Submit the Medication Authorization Request Form?
After submitting the Medication Authorization Request Form, physicians can expect a confirmation and tracking procedures as part of the response process. The review timeframe may vary depending on the insurance policy and medication type.
Next steps typically include awaiting approval notifications and preparing for any additional information requests from insurers.
Common Reasons for Rejection and How to Avoid Them
Several factors can lead to the rejection of a medication authorization request. Common rejection reasons include:
-
Incomplete patient information
-
Lack of required physician signatures
-
Inaccurate diagnosis details
To avoid these issues, double-check all entries and ensure that all required fields are filled out before submission. If a form is rejected, follow the guidelines for amending and resubmitting it promptly.
Security and Compliance When Using the Medication Authorization Request Form
When handling the Medication Authorization Request Form, security is paramount. pdfFiller implements robust security measures, including 256-bit encryption and compliance with HIPAA regulations to protect sensitive health-related documents. It is essential to handle all medical forms with care to maintain patient privacy and data integrity.
Experience the Benefits of pdfFiller for Your Medication Authorization Requests
Utilizing pdfFiller facilitates an efficient and secure method for managing the Medication Authorization Request Form. The platform enhances the form-filling process through features like editing capabilities and electronic signing. By using pdfFiller, physicians can streamline their documentation tasks and manage authorization requests seamlessly.
How to fill out the medication authorization request form
-
1.Access the Medication Authorization Request Form on pdfFiller by searching for its name or using a direct link provided by your healthcare institution.
-
2.Open the form in the pdfFiller editor to access its features designed for easy filling and editing.
-
3.Before you begin, gather all necessary patient information, including the patient’s full name, ID number, diagnosis, and any supporting medical documentation.
-
4.Start filling in the blank fields sequentially, including the patient's information, diagnosis details, and the physician’s signature where required.
-
5.Utilize pdfFiller's interactive elements like checkboxes to ensure all necessary sections are completed. Make sure to double-check that all information entered is accurate and up-to-date.
-
6.Once all fields are filled, review the entire form carefully for any omissions or errors that could affect processing.
-
7.After thorough checks, finalize the document by saving your work. You can download it directly to your device or submit it via fax or an online portal, as specified by your healthcare facility.

Who is eligible to use the Medication Authorization Request Form?
This form is primarily designed for physicians seeking prior authorization for medications like Tysabri on behalf of their patients. It is necessary for healthcare providers operating in Michigan or treating Blue Cross Blue Shield of Michigan members.
Are there any deadlines for submitting the form?
While specific deadlines can vary based on individual insurance agreements, it is important to submit the Medication Authorization Request Form as soon as the need arises to avoid delays in medication access.
What are the accepted submission methods for the form?
The completed Medication Authorization Request Form can be submitted via fax or through an online portal provided by Blue Cross Blue Shield of Michigan or relevant pharmacies as outlined in your practice's submission policy.
What supporting documents are required with this form?
Typically, you'll need to provide detailed patient information, including diagnosis and prior treatment plans. Attach any additional medical documentation that supports the need for the prescribed medication.
What common mistakes should I avoid when filling out the form?
Common mistakes include omitting required patient information, failing to provide a physician's signature, and leaving checkboxes unmarked where necessary. Review all entries carefully before submission.
How long does it take to process the Medication Authorization Request?
Processing times can vary but usually take several days to a week. Be sure to follow up with the insurance provider if you have not received a response by the expected timeframe.
What happens if the authorization request is denied?
If the authorization is denied, you will receive a notification outlining the reasons. Physicians can appeal the decision, often requiring additional documentation to justify the need for the medication.
Related Forms



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.