Last updated on Mar 31, 2026
Get the free Patient Scheduling/Referral Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is patient schedulingreferral form
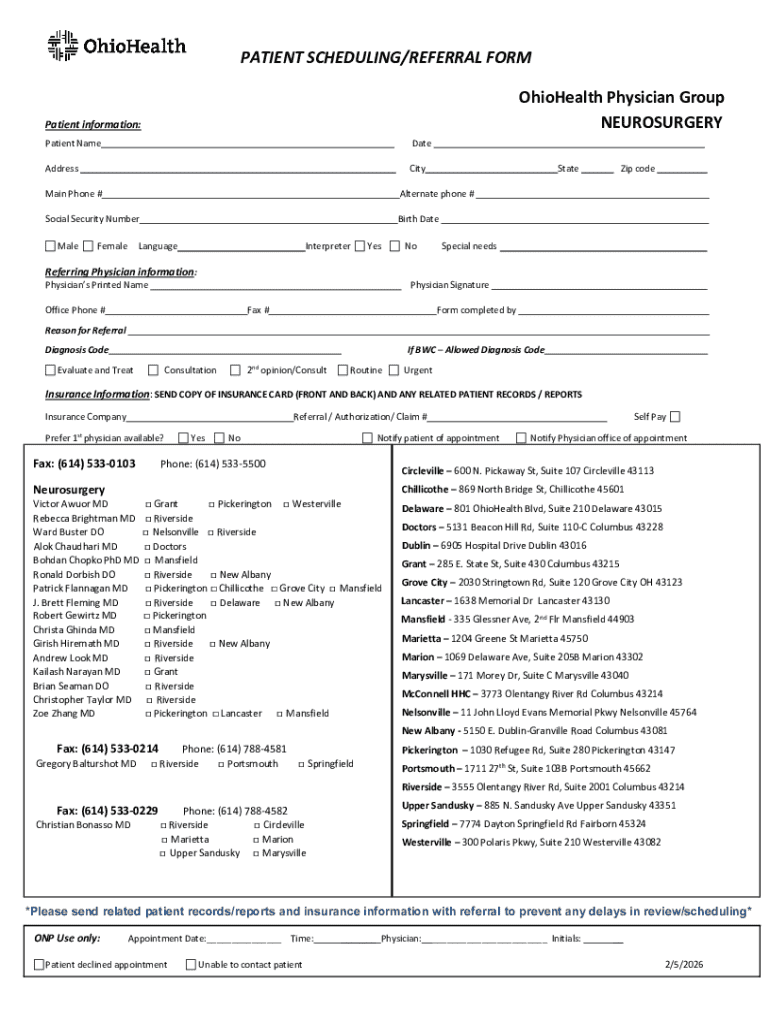
The Patient Scheduling/Referral Form is a healthcare document used by OhioHealth Physician Group to gather patient and referring physician information for scheduling neurosurgery appointments.
pdfFiller scores top ratings on review platforms
Who needs patient schedulingreferral form?
Explore how professionals across industries use pdfFiller.

Patient schedulingreferral form is needed by:
-
Patients seeking neurosurgery appointments
-
Referring physicians in Ohio
-
Healthcare administrators managing patient flow
-
Insurance providers processing claims
-
Medical staff coordinating patient care
Comprehensive Guide to patient schedulingreferral form
What is the Patient Scheduling/Referral Form?
The Patient Scheduling/Referral Form serves as a crucial tool in the patient scheduling process for neurosurgery appointments. This form is designed to gather essential information from patients, referring physicians, and insurance providers, ensuring that all necessary details are collected to facilitate scheduling.
Utilizing this patient scheduling form is imperative for streamlining processes and enhancing the overall efficiency of patient management within healthcare settings.
Purpose and Benefits of the Patient Scheduling/Referral Form
The significance of the patient scheduling form extends to both patients and referring physicians. By streamlining the referral process for neurosurgery, it enhances communication between healthcare providers and reduces the likelihood of delays caused by missing information.
-
Ensures necessary information is provided upfront.
-
Facilitates seamless referrals, promoting timely patient care.
Key Features of the Patient Scheduling/Referral Form
The Patient Scheduling/Referral Form contains specific features that enhance its usability. Among its fillable fields are Patient Name, Address, Social Security Number, and critical insurance information, all designed for ease of completion.
Moreover, it incorporates options for indicating urgency and preferences related to appointment scheduling, making it a comprehensive tool for both patients and referring physicians.
Who Needs to Fill Out the Patient Scheduling/Referral Form?
The audience for this form primarily includes patients seeking referrals for neurosurgery as well as referring physicians who play a pivotal role in initiating the referral process. Understanding who needs to complete this form is essential to ensure that all necessary information is gathered correctly.
Step-by-Step Guide on How to Fill Out the Patient Scheduling/Referral Form Online
Completing the Patient Scheduling/Referral Form effectively involves several steps. Follow this guide to ensure accuracy when filling out the form online:
-
Access the form through pdfFiller.
-
Fill in all required fields, including Patient Name and Address.
-
Review each section for completeness and accuracy.
-
Submit the form according to provided guidelines.
Common Errors and How to Avoid Them When Completing the Form
When filling out the Patient Scheduling/Referral Form, users should be aware of common errors that can delay the process. These often include missing signatures or providing incomplete information.
-
Ensure all sections are filled out completely.
-
Validate the form for accuracy before submitting.
How to Sign or Notarize the Patient Scheduling/Referral Form
The form requires adherence to specific signature requirements, which may include digital or wet signatures. Understanding these differences is essential for proper submission.
For those opting for a digital signature, using pdfFiller to eSign the document is a straightforward process, ensuring compliance and convenience for users.
Submitting the Patient Scheduling/Referral Form: Methods and Guidelines
Once completed, the Patient Scheduling/Referral Form can be submitted via various methods. It can be sent as a paper document, via fax, or submitted online, depending on the specific guidelines provided.
Timely submission is critical, so users should adhere to any associated deadlines for the referral process to avoid delays in scheduling.
Security and Compliance when Using the Patient Scheduling/Referral Form
Data privacy and security are paramount when handling patient information. pdfFiller implements robust security measures that comply with HIPAA and GDPR regulations, safeguarding personal and medical information throughout the process.
Users should understand the importance of these measures in ensuring that their sensitive information remains protected.
Experience Smooth Filling with pdfFiller
pdfFiller offers an efficient environment for completing the Patient Scheduling/Referral Form, featuring easy editing, filling, and eSigning capabilities. Users can enjoy a seamless experience without needing to download any software.
Additonally, pdfFiller provides user support and resources to assist with any issues, enhancing the overall experience for both patients and referring physicians.
How to fill out the patient schedulingreferral form
-
1.Begin by accessing the Patient Scheduling/Referral Form on pdfFiller. Search for the form title in the platform's search bar or navigate through the healthcare forms section to find it.
-
2.Once opened, familiarize yourself with the layout. The form contains various fillable fields, checkboxes, and signature lines that need to be completed accurately.
-
3.Before filling in the form, gather necessary information such as the patient's personal details, including name, address, and Social Security Number, as well as the referring physician's information and insurance details.
-
4.Proceed to fill in the fields sequentially. Enter the patient's name in the designated area and complete the address section. Be sure to fill in the Social Security Number in the appropriate field.
-
5.Utilize checkboxes for gender and, if applicable, indicate the need for a language interpreter. These selections are important for accommodating the patient's needs during their appointment.
-
6.Next, focus on the referring physician's details. This includes entering their name and contact information, ensuring that all spelling is correct to avoid communication issues.
-
7.Once all fields are completed, review the information for accuracy. Double-check each section, ensuring that no required information is missing and that all entries are correct.
-
8.Look for the signature line for the referring physician. Use the e-signature feature on pdfFiller to securely sign the document if required, ensuring compliance with the form's requirements.
-
9.Finalize your form by saving your work regularly. Use the 'Save' feature on pdfFiller to keep changes up to date.
-
10.Once all information is confirmed, download or submit the completed form through pdfFiller. Choose the preferred option—be it downloading for personal records or electronic submission to OhioHealth.

What are the eligibility requirements for submitting this form?
The Patient Scheduling/Referral Form is intended for patients needing neurosurgery and referring physicians who are making the referral. Both parties must provide accurate and valid information on the form.
Is there a deadline for submitting this form?
While there is typically no hard deadline, it is advisable to submit the form as soon as possible to ensure timely scheduling of the neurosurgery appointment. Check with OhioHealth for specific timelines.
How can I submit the completed form?
The completed Patient Scheduling/Referral Form can be submitted electronically through pdfFiller directly to OhioHealth, or it can be printed and mailed as per the referring physician's instruction.
What supporting documents are required with this form?
Along with the Patient Scheduling/Referral Form, you may need to provide insurance information and possibly previous medical records relevant to the referral, depending on the insurance provider's requirements.
What common mistakes should I avoid when filling this form?
Ensure all fields are filled out completely and accurately, especially patient details and insurance information. Failing to provide a signature from the referring physician is another common error.
How long does processing take for this form?
Processing times may vary, but generally expect a few days for the referral to be reviewed and an appointment scheduled. Contact OhioHealth for specific processing inquiries.
Are there any fees associated with this form?
Typically, completing the Patient Scheduling/Referral Form itself does not incur fees. However, medical services related to the appointment may involve costs, which should be verified with the insurance provider.
Related Forms








If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.