Last updated on Apr 10, 2026
Get the free Patient Authorization to Release Protected Health Records
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
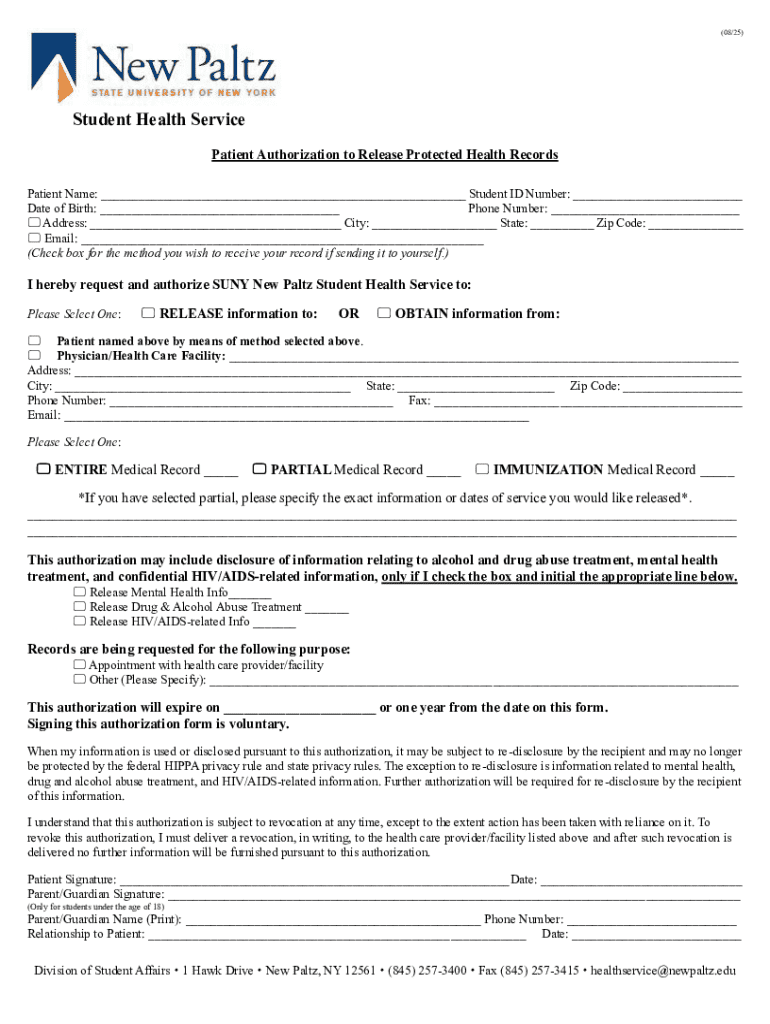
What is patient authorization to release
The Patient Authorization to Release Protected Health Records is a healthcare form used by patients at SUNY New Paltz to authorize the release of their medical records.
pdfFiller scores top ratings on review platforms
Who needs patient authorization to release?
Explore how professionals across industries use pdfFiller.

Patient authorization to release is needed by:
-
Patients seeking to share their health information
-
Parents or guardians of minors needing to authorize record release
-
Healthcare providers requesting patient records
-
Insurance companies verifying medical history
-
Administrative staff handling medical records
Comprehensive Guide to patient authorization to release
What is the Patient Authorization to Release Protected Health Records?
The Patient Authorization to Release Protected Health Records is essential for allowing healthcare providers at SUNY New Paltz to share a patient’s medical records. This form emphasizes patient rights and ensures that the release of health records complies with regulations set forth by HIPAA. Obtaining proper authorization protects patient privacy and ensures that the sharing of sensitive health information is consensual.
Understanding the significance of a patient authorization form is crucial for both patients and healthcare providers. It establishes trust and transparency, allowing patients to manage how their medical information is shared.
Purpose and Benefits of the Patient Authorization to Release Protected Health Records
Patients at SUNY New Paltz need to complete this patient consent form to facilitate the release of their medical records immediately. This process ensures compliance with healthcare privacy laws, reinforcing the commitment to safeguard personal health information.
Moreover, properly filling out a healthcare privacy form helps maintain the confidentiality of health records while allowing legitimate access when necessary.
Who Needs to Complete the Patient Authorization to Release Protected Health Records?
The patient authorization form must be completed by individuals seeking to access health records, which includes both students and their parents or guardians when it involves minors. In circumstances where students require their medical records for various purposes, the completion of this form is essential.
Key roles include:
-
Patients who are over 18 years old must sign the form themselves.
-
Parents or guardians must provide signatures for minors under 18.
How to Fill Out the Patient Authorization to Release Protected Health Records
Filling out the patient authorization to release protected health records involves several steps. First, patients should gather essential information, such as personal identifiers and the recipient's details. Following that, the process can be efficiently completed online using tools like pdfFiller, which simplify the experience.
To complete the online form:
-
Access the pdfFiller platform.
-
Locate the patient authorization form.
-
Fill in the required personal information.
-
Specify the recipient and the details of the records.
-
Review the information for accuracy.
-
Sign and date the form to validate the request.
Key Features of the Patient Authorization to Release Protected Health Records
This form encompasses several crucial sections that facilitate the smooth release of health records. The key features include fillable fields for patient information, recipient details, and specific record requirements. Additionally, it is important to note that the authorization is valid for one year, unless the patient revokes it sooner.
The main sections of the form comprise:
-
Patient personal information fields.
-
Recipient’s details.
-
Record specifics to be released.
Common Errors and How to Avoid Them When Filing the Patient Authorization
When completing the patient authorization form, many individuals may encounter common mistakes that could delay processing. Some frequent errors include incorrect personal information, missing signatures, or improper recipient details.
To prevent these issues:
-
Ensure that all signatures are affixed where necessary.
-
Double-check for data accuracy before submission.
How to Submit the Patient Authorization to Release Protected Health Records
Submission of the patient authorization can be done through multiple methods, catering to the convenience of the patients. Options include online submissions via pdfFiller, mailing the completed form, or handing it in personally at the health service office.
When submitting, it is essential to be aware of any associated processing timelines and fees, if applicable, that may need to be settled at the time of submission.
Security and Compliance Considerations for Submitting the Form
When submitting sensitive documents, security is paramount. pdfFiller implements robust security measures, including 256-bit encryption, ensuring that all submitted health information remains protected. Compliance with HIPAA regulations guarantees that patient data is handled with the utmost care, prioritizing confidentiality.
What to Expect After Submitting the Patient Authorization Form
Upon submission of the patient authorization form, patients can expect to receive confirmation of their request, allowing them to track their submission's status. Should there be any additional steps required to access health records, patients will be informed promptly to ensure seamless follow-up.
Experience the Ease of Completing Your Patient Authorization to Release Protected Health Records with pdfFiller
Utilizing pdfFiller streamlines the completion of the patient authorization form, promoting an efficient and user-friendly experience. Features available include eSigning for easy document execution, editing capabilities to ensure accuracy, and real-time support to address any questions or concerns during the process.
How to fill out the patient authorization to release
-
1.To access the Patient Authorization to Release Protected Health Records form on pdfFiller, navigate to the pdfFiller website and search for the form by its name.
-
2.Once located, click on the form to open it in the pdfFiller editor.
-
3.Before starting, gather your personal information including your full name, address, date of birth, and the details of the recipient who will receive your medical records.
-
4.Using pdfFiller’s interface, fill in the required fields such as your personal information, the recipient's name and contact details, and the specific medical records to be released.
-
5.Utilize the fillable boxes and dropdown menus for ease of navigation, ensuring all necessary information is entered accurately.
-
6.Once you have filled out the form, review the content carefully to ensure all areas are completed correctly and no fields are left blank.
-
7.After reviewing, sign and date the form electronically using pdfFiller’s signature feature.
-
8.To save your work, click the save button in pdfFiller and choose your preferred format for download or submission.
-
9.If you wish to submit the form directly, use the submit button to send it through the methods provided in the system.

Who is eligible to complete this form?
Any patient at SUNY New Paltz who wishes to authorize the release of their protected health records can complete this form. If under 18, a parent or guardian must also sign.
What is the validity period of the authorization?
The authorization granted by this form is valid for one year unless it is revoked earlier by the patient or authorized signer.
How do I submit this authorization form?
You can submit the completed form directly through the pdfFiller platform, download it for manual submission, or send it via email to the designated health service provider.
Are there any required supporting documents?
No specific supporting documents are required to complete this form, but having personal identification information ready will facilitate the process.
What common mistakes should I avoid?
Ensure all required fields are completed, and double-check that your signature is present. Avoid leaving any sections incomplete, as this can delay processing.
How long does it take to process the request?
Processing time may vary based on the health service provider's policies. Generally, it can take a few days to a week, so submit the form early if you need records quickly.
What happens if I change my mind after submitting the form?
If you decide to revoke the authorization, you must do so in writing. Contact the health service provider for their specific revocation process.
Related Forms









If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.