Last updated on Apr 10, 2026
Get the free Primary Care Provider Selection Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is primary care provider selection
The Primary Care Provider Selection Form is a healthcare document used by members to select or change their primary care provider (PCP) under Partnership HealthPlan of California.
pdfFiller scores top ratings on review platforms
Who needs primary care provider selection?
Explore how professionals across industries use pdfFiller.

Primary care provider selection is needed by:
-
Members of Partnership HealthPlan
-
Individuals enrolled in Medi-Cal
-
Patients looking to change their primary care provider
-
Authorized representatives of members
-
Healthcare providers
-
Administrators managing patient enrollments
Comprehensive Guide to primary care provider selection
What is the Primary Care Provider Selection Form?
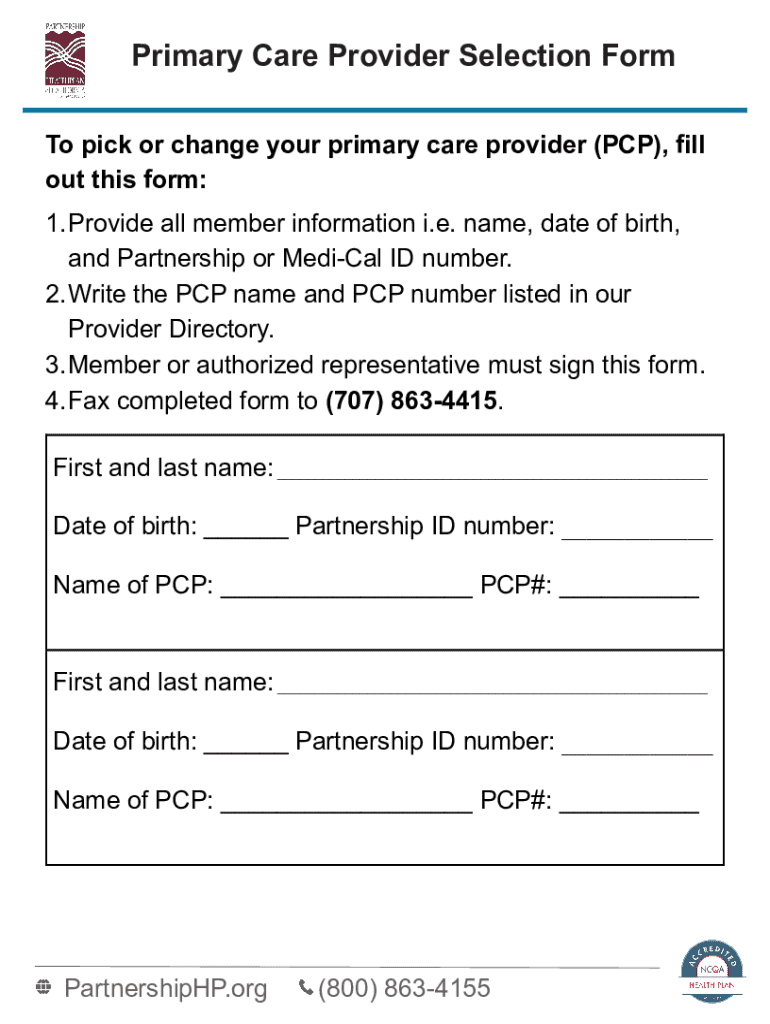
The Primary Care Provider Selection Form is a crucial document used by members of the Partnership HealthPlan of California to select or change their primary care provider (PCP). This form is designed to streamline the process of updating healthcare preferences and ensures members can easily access the medical care they need. Completing the form requires essential member details, such as name, date of birth, and specific information about the chosen PCP, allowing for a seamless transition in healthcare services.
Purpose and Benefits of the Primary Care Provider Selection Form
The primary purpose of the Primary Care Provider Selection Form is to enable members to effectively choose or update their PCP. Utilizing this form offers several benefits, including enhanced access to healthcare services tailored to individual needs and improved continuity of care. Members can ensure they are receiving comprehensive health management by actively maintaining their provider preferences, thus promoting better overall health outcomes.
Who Needs the Primary Care Provider Selection Form?
The Primary Care Provider Selection Form is intended for members of the Partnership HealthPlan or Medi-Cal programs who need to choose a new PCP. While most beneficiaries can utilize this form, it is essential to check for any eligibility restrictions specific to individual circumstances. Common demographics that frequently rely on this form include individuals seeking a change in their healthcare provider due to relocation, dissatisfaction with current services, or the desire for specialized care.
How to Fill Out the Primary Care Provider Selection Form
Filling out the Primary Care Provider Selection Form requires careful attention to detail. Follow these steps to complete the form accurately:
-
Provide your full name and date of birth.
-
Enter your Partnership or Medi-Cal ID number.
-
Select your desired primary care provider by name and number.
-
Sign the form at the designated area.
Common mistakes to avoid include:
-
Leaving any required fields blank.
-
Providing incorrect PCP information.
-
Failure to sign the form.
Common Errors and How to Avoid Them
When filling out the Primary Care Provider Selection Form, users often encounter common pitfalls that can delay processing. Key errors include:
-
Incomplete or inaccurate member information.
-
Forgetting to sign or date the form.
-
Misidentifying the selected PCP.
To ensure a smooth submission, verify all entries are correct and consider double-checking completed forms against provided instructions. By submitting an error-free form, members can expect timely processing and fewer disruptions to their healthcare services.
Submission Methods and Delivery for the Primary Care Provider Selection Form
Members can submit the completed Primary Care Provider Selection Form via several methods, which may include fax, online submission, or by mailing the form to the designated address. It is vital to observe any submission deadlines to ensure timely changes to your PCP are processed. Members should also familiarize themselves with the security measures in place for each submission method to protect personal information during this process.
What Happens After You Submit the Form?
Once the Primary Care Provider Selection Form is submitted, the processing timeline typically varies based on the method of submission. Changes to your PCP will take effect on the first of the month following receipt of the form. To confirm the submission and track any changes in your healthcare provider, users should keep receipts or confirmations received after submission. Maintaining accurate records is essential for managing any healthcare transitions effectively.
How pdfFiller Can Help You Fill Out the Primary Care Provider Selection Form
pdfFiller offers a user-friendly platform to assist members in filling out the Primary Care Provider Selection Form online. Key features include text editing, form creation, and secure eSigning capabilities. The platform also emphasizes security with 256-bit encryption, ensuring compliance with HIPAA and GDPR regulations. This makes pdfFiller a reliable choice for users who prioritize ease of use and data protection while managing their healthcare documents.
Sample or Example of a Completed Primary Care Provider Selection Form
To aid users in completing the Primary Care Provider Selection Form, visual aids or sample forms are available. These samples outline each section of the form, providing notes or explanations to clarify necessary entries. Such resources are instrumental for members who may feel uncertain about how to fill out the California PCPS form accurately.
Make Your Healthcare Choices Easier with pdfFiller
Using pdfFiller streamlines the process of filling out the Primary Care Provider Selection Form, empowering users to make informed healthcare choices. The platform enhances the experience by allowing for easy editing, secure signing, and convenient submission of documents, ensuring that members can effectively manage their healthcare preferences anytime, anywhere.
How to fill out the primary care provider selection
-
1.To access the Primary Care Provider Selection Form on pdfFiller, visit the pdfFiller website and log into your account. If you don’t have an account, you can create one for free to use the form.
-
2.Once logged in, use the search bar to find the 'Primary Care Provider Selection Form' or navigate to the health care forms section to locate it. Click on the form to open it.
-
3.Before you start filling out the form, gather the necessary information such as your name, date of birth, Partnership or Medi-Cal ID number, and your chosen primary care provider's name and number.
-
4.Use pdfFiller’s interface to navigate through the form. Click on each field to input your information. The form requires you to fill in multiple sections, so ensure that all required fields marked with an asterisk (*) are completed.
-
5.If your form contains checkboxes for specific options, click on the relevant boxes to indicate your choices. Review each entry for accuracy before proceeding.
-
6.Once you’ve filled out the form, carefully review all provided information. Ensure that your PCP choice is correctly entered and that there's a valid signature section filled out.
-
7.To finalize the form, use the 'Finish' button on pdfFiller. You have options to save or download your completed form in various formats. Choose 'Save As PDF' or 'Download' to keep a copy.
-
8.If you need to submit the form, check the instructions provided on where to fax or send it. Use the output options on pdfFiller to send it directly or save it for faxing later.

Who is eligible to use the Primary Care Provider Selection Form?
Eligibility is for members of the Partnership HealthPlan, including individuals enrolled in Medi-Cal. If you are a member or an authorized representative, you can complete this form to select or change a primary care provider.
Are there any deadlines for submitting this form?
There are no strict deadlines; however, it is advisable to submit the form before the first day of the month to ensure that changes take effect on the first of the following month after submission.
How do I submit the completed Primary Care Provider Selection Form?
You can submit the completed form by faxing it to the number provided in the form instructions. Ensure that the form is signed before faxing it to validate the change of your primary care provider.
What supporting documents do I need to include?
Typically, no additional documents are required to accompany this form. It primarily requires your personal identification information and your selected PCP's name. Ensure that all information is filled out as requested.
What common mistakes should I avoid when filling out the form?
Common mistakes include not signing the form, leaving required fields blank, and entering incorrect personal information such as your ID number. Double-check all entries before submission to avoid delays.
How long does it take for changes to take effect?
Changes to your primary care provider typically take effect on the first day of the month following the receipt of your completed form by the health plan. Early submission can expedite this process.
What should I do if I need assistance filling out the form?
If you require assistance, consider contacting customer service for Partnership HealthPlan. They can provide guidance on filling out the form correctly and help resolve any questions or issues you may have.
Related Forms










If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.