Last updated on Oct 29, 2015
Get the free Health Provider Questionnaire
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
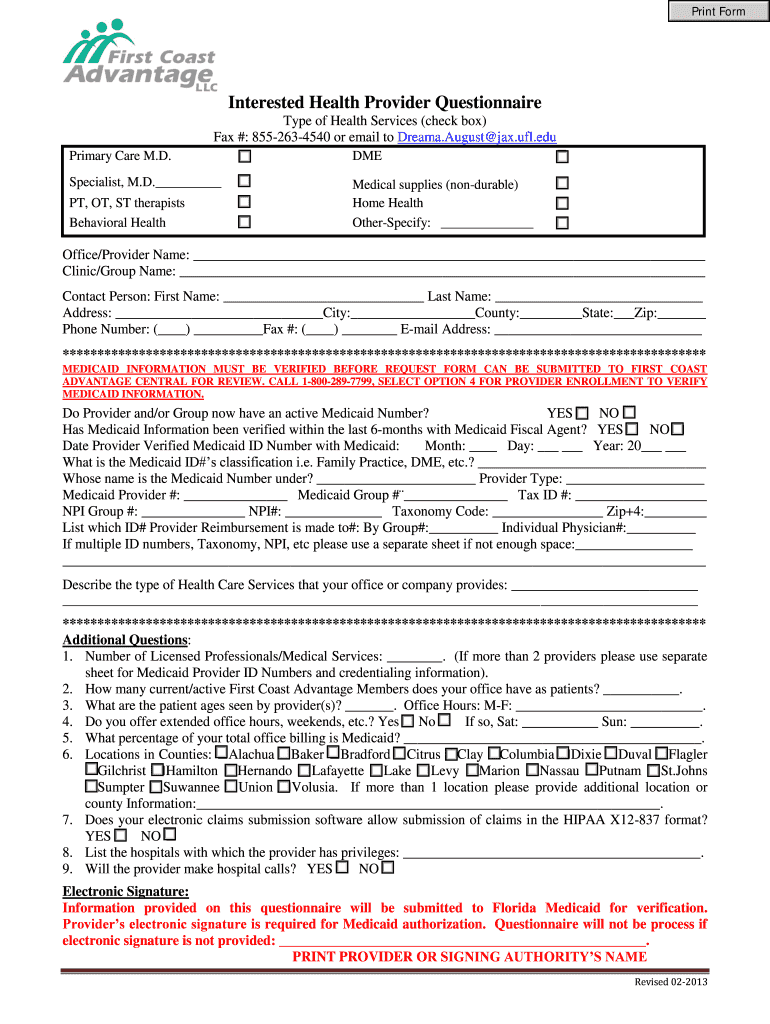
What is Provider Questionnaire
The Health Provider Questionnaire is a healthcare form used by providers to submit information for Medicaid verification in Florida.
pdfFiller scores top ratings on review platforms
Who needs Provider Questionnaire?
Explore how professionals across industries use pdfFiller.

Provider Questionnaire is needed by:
-
Healthcare providers in Florida
-
Medicaid applicants
-
Administrative staff managing healthcare forms
-
Medical billing professionals
-
Insurance representatives
-
Practices providing Medicaid services
Comprehensive Guide to Provider Questionnaire
What is the Health Provider Questionnaire?
The Health Provider Questionnaire is an essential document for healthcare providers participating in Medicaid in Florida. It serves as a formal means for providers to submit their information for Medicaid verification.
This questionnaire plays a crucial role in ensuring that all necessary details are collected efficiently, which helps verify eligibility and compliance. To submit the form, providers are required to include an electronic signature, confirming the authenticity of the information provided.
Benefits of Using the Health Provider Questionnaire
Completing the Health Provider Questionnaire offers numerous advantages for health providers looking to enroll or reverify for Medicaid. One significant benefit is the streamlined process it provides, making Medicaid verification much more efficient.
Additionally, utilizing this healthcare provider questionnaire ensures that providers remain compliant with state regulations. The clear format of the form aids providers in organizing the necessary information without confusion.
Key Features of the Health Provider Questionnaire
The Health Provider Questionnaire is designed with user-friendliness and compliance in mind. Its components include various checkboxes and blank fields that allow healthcare providers to easily input their information.
-
Required fields include office/provider name and Medicaid credentials.
-
An electronic signature line is included, which is vital for the submission process.
Who Needs to Complete the Health Provider Questionnaire?
Health care providers in Florida who are looking to enroll or reverify for Medicaid are required to complete the Health Provider Questionnaire. Understanding the eligibility criteria is essential for providers to ensure their compliance and successful submission.
Typically, various types of providers need this Florida Medicaid form to confirm their participation in the Medicaid program.
How to Fill Out the Health Provider Questionnaire Online
To effectively complete the Health Provider Questionnaire, follow this step-by-step guide while using pdfFiller.
-
Start by accessing the form through the pdfFiller platform.
-
Carefully fill out each section, paying attention to field labels.
-
Use the tips provided to ensure common fields are filled out accurately.
-
Complete the electronic signature section as required.
Submission Guidelines for the Health Provider Questionnaire
Submitting the completed Health Provider Questionnaire can be done through various methods. Providers can submit the form online or via mail, depending on their preference.
It is crucial to be aware of important deadlines and the anticipated processing times for Medicaid verification. After submission, providers can receive confirmation and track their submissions to ensure everything is in order.
Common Errors and Solutions When Completing the Health Provider Questionnaire
Many users encounter common mistakes when filling out the Health Provider Questionnaire. Some frequent errors include missing information and incorrect signatures.
-
Review the form thoroughly before submission to avoid omitting any details.
-
Ensure the electronic signature is correctly applied to validate the document.
Utilizing validation tools or checklists can help providers confirm that their forms are completed accurately.
Security and Compliance for Submitting the Health Provider Questionnaire
Understanding the security measures in place during the submission of the Health Provider Questionnaire is crucial for protecting sensitive information. The form must comply with various regulations, including HIPAA, to safeguard users' data.
pdfFiller employs robust security protocols, including 256-bit encryption, to ensure the safe handling of the questionnaire. This level of diligence helps healthcare providers feel confident about the security of their submitted information.
Using pdfFiller to Complete the Health Provider Questionnaire
pdfFiller offers a user-friendly platform for filling out the Health Provider Questionnaire, making the process simpler and more accessible. Users can take advantage of various capabilities like editing, eSigning, and cloud storage to enhance their experience.
To use pdfFiller for this specific form, providers can easily access it online and utilize its features for a seamless completion and submission process.
Next Steps After Submission of the Health Provider Questionnaire
After submitting the Health Provider Questionnaire, providers should be aware of the confirmation process and the expected timelines for response. It is important to keep track of the application status to address any issues that may arise.
In the event that renewal or resubmission is necessary, providers should follow the outlined guidelines to ensure they maintain compliance with Medicaid requirements.
How to fill out the Provider Questionnaire
-
1.Access the Health Provider Questionnaire on pdfFiller by searching for it in the forms library or by entering the URL directly in your web browser.
-
2.Once the form loads, review the layout and familiarize yourself with the sections that need to be completed.
-
3.Before starting, gather necessary information such as your office/provider name, types of health services offered, and Medicaid credentials to ensure a smooth filling process.
-
4.Begin filling out the form by clicking on the first blank field or checkbox. Use the text tools to enter your provider information accurately.
-
5.Answer all relevant questions about your practice, checking the appropriate boxes for the types of health services provided.
-
6.If there are sections that require documentation, ensure you have those documents ready to refer to as you complete the form.
-
7.Once all fields are completed, carefully review the information for accuracy and completeness, correcting any mistakes as needed.
-
8.Locate the electronic signature line and use the pdfFiller tools to add your digital signature, which is necessary for Medicaid authorization.
-
9.After signing, save your progress regularly to avoid data loss by selecting the 'Save' option in pdfFiller.
-
10.Once you have reviewed the final version and confirmed all entries are correct, choose the 'Download' option to save a copy of the completed form to your device.
-
11.Alternatively, submit the form directly through pdfFiller by following the submission process indicated for Medicaid forms, or by downloading and submitting it as required by the specific Medicaid program instructions.

Who is eligible to fill out the Health Provider Questionnaire?
Healthcare providers who offer Medicaid services in Florida are eligible to fill out the Health Provider Questionnaire. It is critical for those seeking Medicaid verification to ensure that their provider information is accurately represented.
What is the deadline for submitting the Health Provider Questionnaire?
While specific deadlines may vary, it is typically important to submit the Health Provider Questionnaire as soon as possible to avoid delays in Medicaid authorization. Check with your local Medicaid office for any specific timelines.
What are acceptable submission methods for this form?
The Health Provider Questionnaire can be submitted electronically via pdfFiller or downloaded for physical submission. Make sure to follow the guidelines provided by your local Medicaid office for the preferred submission method.
Are there any supporting documents required for the Health Provider Questionnaire?
Yes, you may need to provide additional documents such as proof of Medicaid credentials or other relevant certifications when submitting the Health Provider Questionnaire. Always check local requirements for specifics.
What common mistakes should I avoid when filling out this form?
Common mistakes include entering incorrect or incomplete information, failing to provide a digital signature, and not reviewing the form before final submission. Ensure that all sections are thoroughly completed to avoid processing delays.
How long does it take to process the Health Provider Questionnaire?
Processing times can vary, but typically, you can expect a turnaround of several business days once the questionnaire is submitted. Check with your Medicaid office for specific timelines.
What if I have questions while filling out the Health Provider Questionnaire?
If you have questions while filling out the form, it’s advisable to consult your office administration team or contact your local Medicaid office for guidance, ensuring that you approach the form accurately.
Related Forms








If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.