Last updated on Nov 4, 2015
Get the free Health Care Provider Application Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Healthcare Provider Application
The Health Care Provider Application Form is a business document used by healthcare professionals to apply for insurance coverage.
pdfFiller scores top ratings on review platforms
Who needs Healthcare Provider Application?
Explore how professionals across industries use pdfFiller.

Healthcare Provider Application is needed by:
-
Healthcare providers seeking insurance
-
Insurance agents assisting applicants
-
Medical business owners applying for coverage
-
Practitioners needing professional liability insurance
-
Healthcare organizations procuring insurance
Comprehensive Guide to Healthcare Provider Application
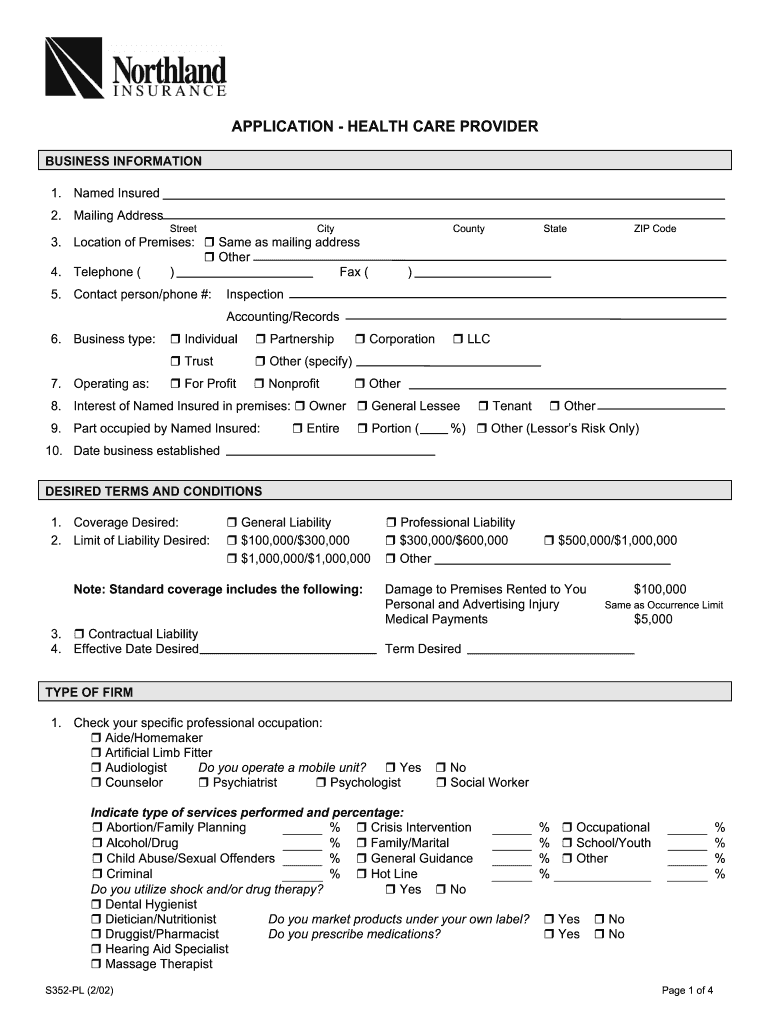
What is the Health Care Provider Application Form?
The Health Care Provider Application Form is essential for healthcare professionals seeking insurance coverage. This form collects vital information, including the type of healthcare services offered and the applicant's business structure. Understanding its significance helps ensure that healthcare providers secure necessary coverage, thereby protecting both them and their patients.
When filling out the form, specific details such as Named Insured, Mailing Address, Business Type, and Coverage Desired must be accurately provided. These elements facilitate effective processing and approval of claims.
Purpose and Benefits of the Health Care Provider Application Form
The Health Care Provider Application Form is crucial for ensuring that healthcare professionals can obtain appropriate insurance coverage. This coverage not only protects providers against liability but also instills confidence in patients seeking medical care.
Using platforms like pdfFiller simplifies the application submission process. Its user-friendly interface allows for convenient form filling and enhances the overall efficiency of submitting healthcare professional insurance applications.
Who Needs the Health Care Provider Application Form?
The application form is tailored for various healthcare professionals. Solo practitioners, clinics, and large healthcare facilities can all benefit from completing this important document.
Not having appropriate insurance can lead to significant risks for providers. By applying for coverage, healthcare professionals can avoid potential financial pitfalls and ensure compliance with regulatory requirements.
Key Features of the Health Care Provider Application Form
Key components of the Health Care Provider Application Form include essential fields such as Named Insured, Mailing Address, Business Type, and Coverage Desired. Attention to these critical fields is necessary when completing the form.
-
Named Insured: Identifies the individual or entity applying for coverage.
-
Mailing Address: Where communication regarding the application will be sent.
-
Business Type: Specifies the structure of the healthcare practice.
-
Coverage Desired: Outlines the type of coverage the provider is seeking.
Completing these sections with precise information streamlines the processing of applications.
How to Fill Out the Health Care Provider Application Form Online
Filling out the Health Care Provider Application Form online can be accomplished in a few simple steps. First, start by accessing the form through pdfFiller, where you can break down each section for clarity.
-
Begin with the Named Insured section by entering your name or business title.
-
Provide a comprehensive Mailing Address that ensures proper delivery of correspondence.
-
Indicate your Business Type, ensuring to check the applicable options.
-
Specify your Coverage Desired to align with your practice needs.
To avoid common errors, double-check each field and utilize available digital tools within pdfFiller for an optimized experience.
Digital Signature Requirements for the Health Care Provider Application Form
Signing the Health Care Provider Application Form is a vital step, as it requires both an applicant's and producing agent's signatures. Understanding the difference between digital and wet signatures can aid in this process.
Digital signatures provide a secure method to sign documents electronically and are legally recognized in the healthcare sector. To eSign using pdfFiller, follow the provided instructions to ensure compliance and validation.
Submission Methods and Delivery for the Health Care Provider Application Form
Once the Health Care Provider Application Form is completed, several submission methods are available. You can choose to submit via email or physical mail, depending on your preference.
-
Email submissions for immediate processing.
-
Physical mail for traditional delivery methods.
It is advisable to track your submissions to confirm receipt and monitor the process. Be mindful of any associated fees and estimated processing times that may impact your application.
What Happens After You Submit the Health Care Provider Application Form?
After submitting the form, applicants can expect a typical processing timeline. It’s important to know how to check the status of your application effectively.
-
Contact the insurer to inquire about application progress.
-
Be prepared for possible delays or rejections due to missing information or discrepancies.
Understanding these factors can help manage expectations during the waiting period.
Security and Compliance of the Health Care Provider Application Process
Security is paramount when submitting sensitive data in the Health Care Provider Application Process. pdfFiller employs robust security features, including 256-bit encryption, ensuring the protection of personal information.
Compliance with HIPAA and GDPR regulations highlights the importance of safeguarding sensitive health data throughout the application process. pdfFiller’s data retention practices further support user privacy and confidentiality.
Streamline Your Application Process with pdfFiller
Utilizing pdfFiller significantly enhances the application experience for healthcare providers. The platform's intuitive design allows users to edit, fill, and eSign forms efficiently while ensuring document safety.
Cloud-based document management provides healthcare professionals with seamless access and management of their applications. Start your application journey today by accessing the form through pdfFiller for a straightforward experience.
How to fill out the Healthcare Provider Application
-
1.To access the Health Care Provider Application Form on pdfFiller, navigate to the pdfFiller website and use the search bar to find the form by name.
-
2.Once you locate the form, click on it to open the interactive PDF editor, which allows you to fill in the required fields easily.
-
3.Before you start completing the form, gather all necessary information, including your business structure, type of healthcare services you provide, coverage limits desired, and professional qualifications.
-
4.As you fill in the fields, use the tools within pdfFiller, such as text boxes, checkboxes, and dropdown menus, to input your information accurately.
-
5.Be aware of sections like 'Named Insured', 'Mailing Address', and 'Coverage Desired', ensuring all information is filled out completely.
-
6.Once you have completed the form, carefully review all entries for accuracy. It’s important to check for any missed fields or errors in your information.
-
7.After reviewing, finalize your document by saving your changes within pdfFiller. You can download the completed form to your device for your records or submit it directly via pdfFiller’s submission options.

Who is eligible to complete the Health Care Provider Application Form?
Eligibility to complete the Health Care Provider Application Form includes any licensed healthcare professional or business that offers healthcare services and is seeking insurance coverage.
What documents do I need to submit with the application?
Typically, you will need to provide evidence of your professional qualifications, business structure, and any relevant certifications along with the completed application form.
Are there deadlines for submitting this application?
While specific deadlines can vary by insurance provider, it's advisable to submit your application as soon as possible to ensure timely processing and coverage.
How can I submit the completed form?
You can submit the completed Health Care Provider Application Form through pdfFiller’s direct submission options or download it for physical submission to your chosen insurance provider.
What are common mistakes to avoid when filling out the form?
Common mistakes include missing mandatory fields, incorrect information related to coverage, and improper signatures from the applicant or producing agent.
How long does processing take after submission?
Processing times can vary widely based on the insurance provider but generally expect a timeframe of 2-4 weeks depending on their review process.
Can I make edits to the form after submission?
Generally, once the form is submitted, no further edits can be made. To correct any errors, you would need to contact the insurance provider directly.
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.