Last updated on Dec 17, 2015
Get the free Authorization to Disclose Medical Information
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
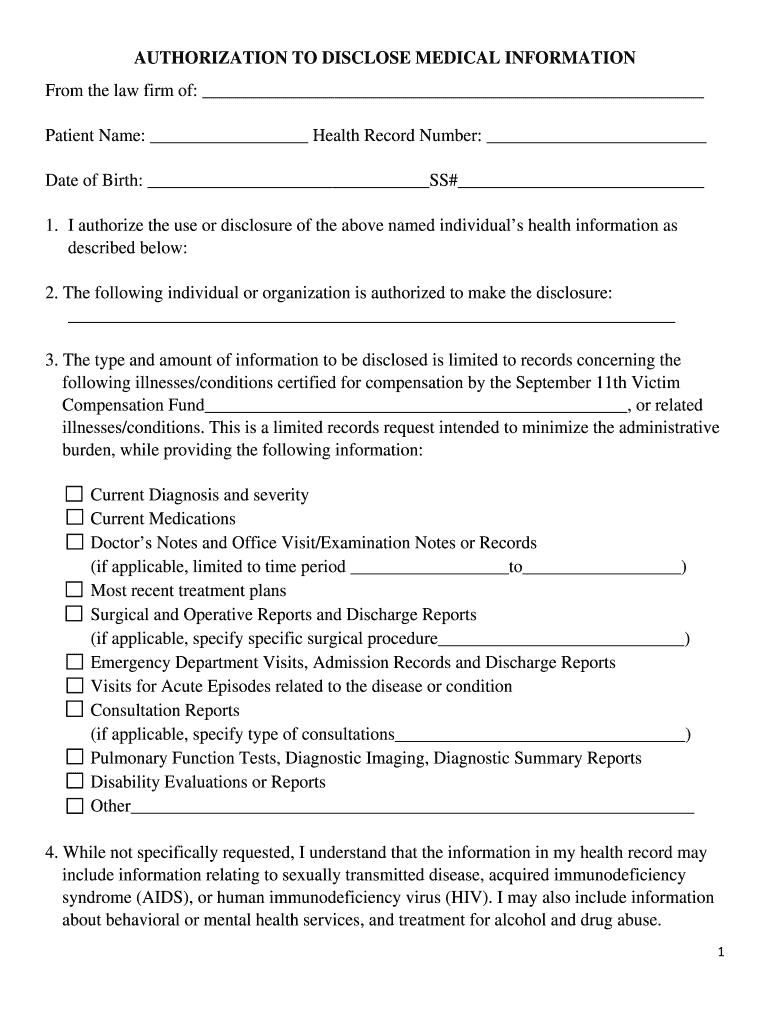
What is Medical Disclosure Authorization
The Authorization to Disclose Medical Information is a medical records release form used by patients to permit the release of their health information for claims related to the September 11th Victim Compensation Fund.
pdfFiller scores top ratings on review platforms
Who needs Medical Disclosure Authorization?
Explore how professionals across industries use pdfFiller.

Medical Disclosure Authorization is needed by:
-
Patients seeking to disclose their health records
-
Claimants applying for the September 11th Victim Compensation Fund
-
Healthcare providers facilitating the disclosure
-
Legal representatives or advocates assisting claimants
-
Witnesses verifying the authorization
-
Organizations managing claims related to medical information
Comprehensive Guide to Medical Disclosure Authorization
What is the Authorization to Disclose Medical Information?
The Authorization to Disclose Medical Information is a vital form that permits the release of a patient's health information to specified individuals or organizations. This form significantly impacts healthcare claims, especially concerning the September 11th Victim Compensation Fund. It covers various types of medical records, including important details such as diagnoses, medications, and treatment plans.
By utilizing this medical disclosure authorization form, patients ensure that the necessary medical information is available for their claims. Understanding its purpose is essential for both patients and healthcare providers.
Purpose and Benefits of Using the Authorization to Disclose Medical Information
Individuals may need to complete this form to facilitate the release of their medical records for claims processing. Completing the HIPAA medical release form not only safeguards patient privacy but also ensures essential health information is accessible for claim evaluations. Compliance with HIPAA regulations is paramount, protecting patient health information throughout the process.
Benefits of using this authorization include expedited claims processing and the reassurance that all necessary documentation can be obtained without compromising patient confidentiality.
Who Needs the Authorization to Disclose Medical Information?
The primary users of this form include claimants and witnesses involved in the claims process. Situations that necessitate this authorization may arise during the filing of claims for various purposes, including medical reimbursements or compensation claims.
Having a witness sign the authorization is crucial, as it can validate the process and ensure that the information disclosed is accurate, thus preventing disputes in the future.
How to Fill Out the Authorization to Disclose Medical Information: Step-by-Step Guide
Completing the authorization form accurately requires attention to detail. Follow these steps to ensure proper submission:
-
Fill in the claimant's personal information, including name and contact details.
-
Specify the information being disclosed by checking applicable boxes.
-
Provide the names of individuals or organizations authorized to receive the records.
-
Ensure both the claimant and the witness sign and date the form appropriately.
-
Double-check all filled fields to prevent errors.
In complex situations involving multiple medical record sources, include clear instructions on which records are required to avoid delays in processing.
Common Errors When Completing the Authorization to Disclose Medical Information
Many users encounter frequent mistakes while filling out the medical records release form. Common pitfalls include missing signatures, incorrectly checked boxes, and incomplete information. To avoid these errors, consider the following tips:
-
Review each section thoroughly before submission.
-
Confirm that both the claimant and witness sign the document.
-
Utilize validation checks available on the form if applicable, to ensure accuracy.
By avoiding these mistakes, claimants can streamline the submission process and enhance the likelihood of prompt approvals.
Submission and Processing of the Authorization to Disclose Medical Information
After completing the authorization form, it is essential to submit it correctly. Submit the completed authorization form through designated channels, which may include mailing or electronically submitting it, depending on specific guidelines provided by the healthcare provider or relevant organizations.
Processing times can vary, so it's crucial to inquire about expected timelines and any fees associated with filing. Claimants should also seek confirmation and tracking methods for their submissions to ensure peace of mind.
Security and Compliance: Protecting Your Information with pdfFiller
pdfFiller prioritizes security measures when handling sensitive health information on the Authorization to Disclose Medical Information form. With robust security protocols compliant with HIPAA and GDPR regulations, users can feel confident that their personal data is protected.
Utilizing a trusted platform like pdfFiller ensures not only security but also a streamlined experience in managing the authorization form and its associated processes.
Using pdfFiller to Complete Your Authorization to Disclose Medical Information
pdfFiller simplifies the process of editing and filling out the authorization form. Its user-friendly interface allows for easy creation, signing, and submission of the form online, removing the stress of manual paperwork. Key features include pre-fill options that save time and document-sharing capabilities for collaborative completion.
Using pdfFiller enhances usability, enabling users to manage their forms efficiently and securely.
Importance of a Completed Authorization for Claims Processing
Submitting a claim without the Authorization to Disclose Medical Information can lead to delays and complications in the processing of claims related to the September 11th Victim Compensation Fund. This authorization is essential for facilitating necessary health information disclosures, ensuring a smooth claims process.
Understanding the importance of this medical release is crucial for claimants aiming for timely and effective claims processing.
Ready to Get Started? Fill Out Your Authorization to Disclose Medical Information Today
Individuals can take immediate action by completing the form using pdfFiller for a streamlined process. The platform offers additional support features to assist users throughout the form completion, ensuring both security and efficiency in handling sensitive health information.
How to fill out the Medical Disclosure Authorization
-
1.Access pdfFiller and search for 'Authorization to Disclose Medical Information' in the template library.
-
2.Click on the form to open it in the pdfFiller editor where you can fill out the necessary fields.
-
3.Before starting, gather all relevant information including the patient's details, types of information to be disclosed, and the names of individuals or organizations receiving the records.
-
4.Begin filling in the patient's name, contact details, and any identification numbers required.
-
5.Next, specify the types of health information that can be shared, such as diagnoses, medications, and treatment plans.
-
6.Ensure all fillable fields are completed clearly and accurately, utilizing checkboxes where applicable.
-
7.Review the completed form carefully to ensure all information is correct and no fields are left unfinished.
-
8.Once reviewed, proceed to sign the form electronically in the designated signing area.
-
9.Have a witness sign the form as well, ensuring their details are also entered where required.
-
10.After signing and confirming all necessary information is accurate, utilize the 'Save' option to keep a copy on your device.
-
11.You can download the form by clicking the download button or submit it directly through the platform if that option is available.
-
12.Maintain a copy of the completed form for your records and ensure it is submitted to the appropriate organization or individual.

Who is eligible to use the Authorization to Disclose Medical Information form?
Any patient seeking to authorize the release of their medical information for claims related to the September 11th Victim Compensation Fund is eligible to use this form.
Are there specific deadlines for submitting this form?
While this form does not have a specific deadline, timely submission is crucial for the processing of claims related to the September 11th Victim Compensation Fund.
How do I submit the completed Authorization to Disclose Medical Information form?
The completed form can be submitted via mail or electronically, depending on the requirements set by the organization handling your claim.
What supporting documents may be required with this form?
Typically, no additional documents are needed beyond the completed form itself, but it's advisable to check the specific requirements of the organization requiring the authorization.
What are common mistakes to avoid when completing this form?
Common mistakes include leaving fields blank, not providing clear information about the types of disclosures, and missing signatures from both the patient and witness.
How long does it take to process the Authorization to Disclose Medical Information form?
Processing times can vary, but once submitted, allow a few weeks for the organization to process your authorization and share the medical records requested.
What should I do if I made a mistake after submitting the form?
If you realize there's an error after submission, contact the organization managing your claim immediately to rectify the information as soon as possible.
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.