Last updated on Jan 18, 2016
Get the free Patient Medical History Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
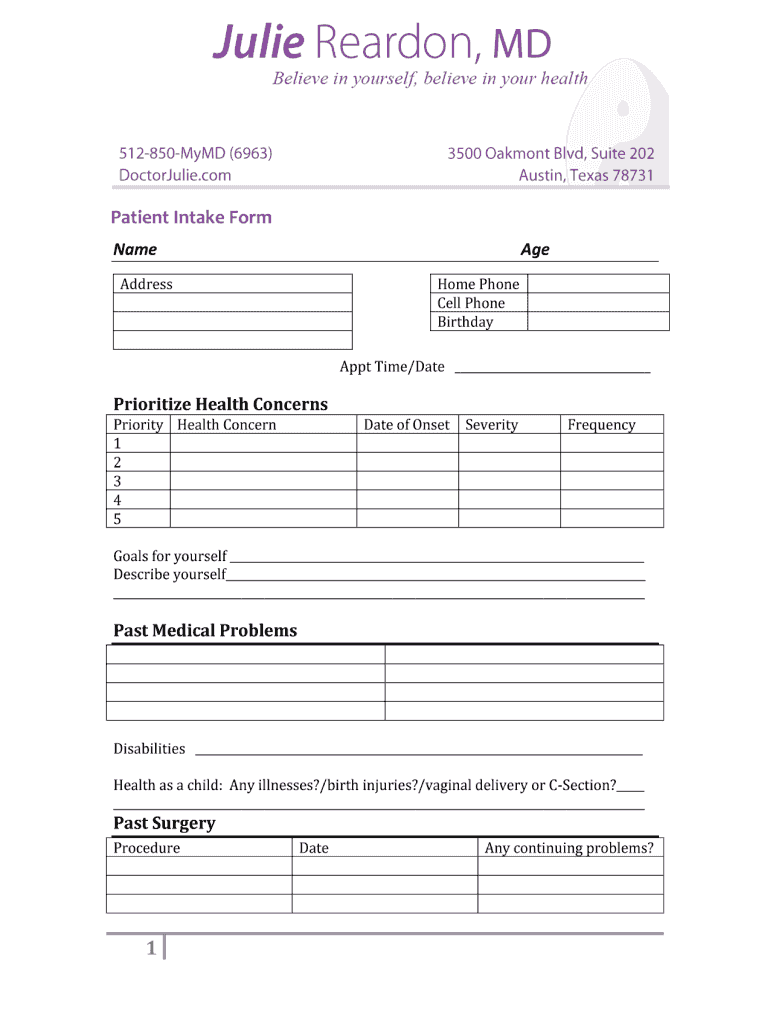
What is Medical History Form
The Patient Medical History Form is a healthcare document used by providers to collect essential information about a patient's medical history.
pdfFiller scores top ratings on review platforms
Who needs Medical History Form?
Explore how professionals across industries use pdfFiller.

Medical History Form is needed by:
-
Healthcare providers for patient intake processing
-
Patients to detail their medical conditions
-
Medical assistants to prepare for patient consultations
-
Insurance companies for claims assessment
-
Family members assisting patients with health documentation
Comprehensive Guide to Medical History Form
What is the Patient Medical History Form?
The Patient Medical History Form is a critical document utilized by healthcare providers to compile detailed information regarding a patient's medical history. This form serves various purposes, including aiding in accurate diagnosis and effective treatment. It collects essential information such as allergies, current medications, family health history, and lifestyle choices.
Different types of patients may need to fill out this form, including new patients registering for the first time and individuals with existing health concerns. By obtaining comprehensive data through a medical history template, healthcare professionals can provide better-informed care tailored to individual needs.
Purpose and Benefits of the Patient Medical History Form
The primary purpose of the Patient Medical History Form is to assist healthcare providers in diagnosing and treating conditions effectively. A comprehensive medical history is vital for understanding a patient's health landscape, enabling providers to identify patterns and make more informed decisions.
Benefits for patients include personalized care that targets specific health issues, leading to improved treatment efficiency. Utilizing a patient health questionnaire allows for quick assessments, ensuring no essential details are overlooked during the diagnostic process.
Key Features of the Patient Medical History Form
This form comprises several key components that streamline data collection, including sections for allergies, current medications, family health history, and lifestyle concerns. Additional fields or checkboxes enhance user experience by making it easier for patients to provide accurate information.
Moreover, the form has customizable options to cater to specific healthcare needs, making it adaptable for varied practices, thus allowing healthcare providers to design their medical history questionnaire according to their unique requirements.
Who Needs the Patient Medical History Form?
The Patient Medical History Form is essential for various demographics, primarily new patients who are visiting a healthcare provider for the first time. Additionally, any individual with ongoing health issues or who is seeking treatment for an ailment may be asked to complete this document.
Healthcare providers might request this form in situations such as routine check-ups, before surgical procedures, or during the intake process for specialized care. Its relevance spans all age groups, making it a necessary element in pediatric, adult, and geriatric care.
How to Fill Out the Patient Medical History Form Online (Step-by-Step)
Filling out the Patient Medical History Form online involves a straightforward process. Follow these steps:
-
Access the form through the designated platform.
-
Begin by entering personal information, including name and contact details.
-
Complete each section thoroughly, particularly those concerning medications and allergies.
-
Review the information for accuracy before submission.
-
Submit the form electronically or by the preferred submission method.
Common mistakes to avoid include omitting important details and providing vague responses. Ensure clarity and precision to aid healthcare providers in delivering optimal care.
Submission Methods and Delivery of the Patient Medical History Form
Once you have completed the Patient Medical History Form, several submission methods are available. Users can choose to submit the form electronically or via traditional methods, such as mailing a hard copy. If using pdfFiller, electronic submission options are available, making the process more efficient.
For best practices, it's recommended to follow up on submissions to confirm receipt. This ensures that healthcare providers have the necessary information for patient care.
Security and Compliance for the Patient Medical History Form
Data security is a significant concern when handling sensitive medical information. The Patient Medical History Form must be managed following strict security measures. pdfFiller employs 256-bit encryption and adheres to compliance standards such as HIPAA and GDPR to ensure that user data remains protected.
Privacy concerns are addressed through various strategies that pdfFiller implements, allowing users to confidently manage their healthcare forms without fear of unauthorized access to their personal information.
Sample or Example of a Completed Patient Medical History Form
To assist users in completing their own forms, a sample of a filled-out Patient Medical History Form is available for reference. This illustrative example demonstrates how to approach common sections, such as medications and family health history, providing clarity on what constitutes thorough completion.
Focus on accuracy and completeness when filling out each section, as this information plays a critical role in patient care.
Getting Started with pdfFiller for Your Patient Medical History Form
pdfFiller offers users valuable tools to simplify the completion of the Patient Medical History Form. With features like form fillability, eSigning, and comprehensive document management, users can navigate the process seamlessly.
Getting started with pdfFiller is straightforward, providing access to tools that enhance the user experience for both this form and others within the healthcare documentation suite.
How to fill out the Medical History Form
-
1.To access the Patient Medical History Form on pdfFiller, visit the homepage and use the search bar to find the form by name. Click on the form title to open it in the editor.
-
2.Once the form is open, familiarize yourself with the interface, which includes easy navigation tools for scrolling through each section.
-
3.Before starting to fill out the form, gather relevant medical information, including details on allergies, medications, family medical history, and lifestyle choices to ensure accuracy.
-
4.Begin filling in the form by clicking on each blank field. Use the provided checkboxes where applicable for quick selections concerning allergies and medications.
-
5.Provide detailed answers in the open fields, particularly for sections requiring more context, like family history or lifestyle concerns.
-
6.After completing the form, review your entries carefully to ensure all information is accurate and up-to-date, checking for any missed sections.
-
7.Once you are satisfied with your input, utilize the save function to store your progress or use the download option to save a copy of the form to your device.
-
8.If needed, you can submit the filled form electronically through the submission feature on pdfFiller, which typically allows for direct emailing or sharing through links.

Who is eligible to fill out the Patient Medical History Form?
The Patient Medical History Form is designed for use by patients receiving healthcare services and their healthcare providers. Any person seeking medical attention or advice can complete this form.
What information is typically required to complete the form?
You will need to provide information about any allergies, current medications, family health history, lifestyle habits, and any past medical conditions. Gathering this information in advance will facilitate completion.
How do I submit the completed Patient Medical History Form?
After filling out the form on pdfFiller, you can submit it electronically directly through the platform. Alternatively, you can download the completed form and provide it to your healthcare provider in person or via email.
What are common mistakes to avoid when filling out the form?
Common mistakes include leaving fields blank, providing outdated information, and not double-checking for spelling errors. Ensure all sections are completed accurately for the best outcome.
How long does it take to process the Patient Medical History Form?
Processing time can vary, but typically, once submitted online, healthcare providers can review the form immediately or within a few hours. Check with your provider for their specific timelines.
Is notarization required for the Patient Medical History Form?
No, notarization is not required for the Patient Medical History Form. It is a standard healthcare document used for information gathering only.
Can family members fill out the form for the patient?
Yes, family members can assist patients in filling out the Patient Medical History Form, especially if the patient has difficulty providing the necessary information themselves.
Related Forms








Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.