Last updated on May 20, 2026
GSA SF 1169 1977-2026 free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
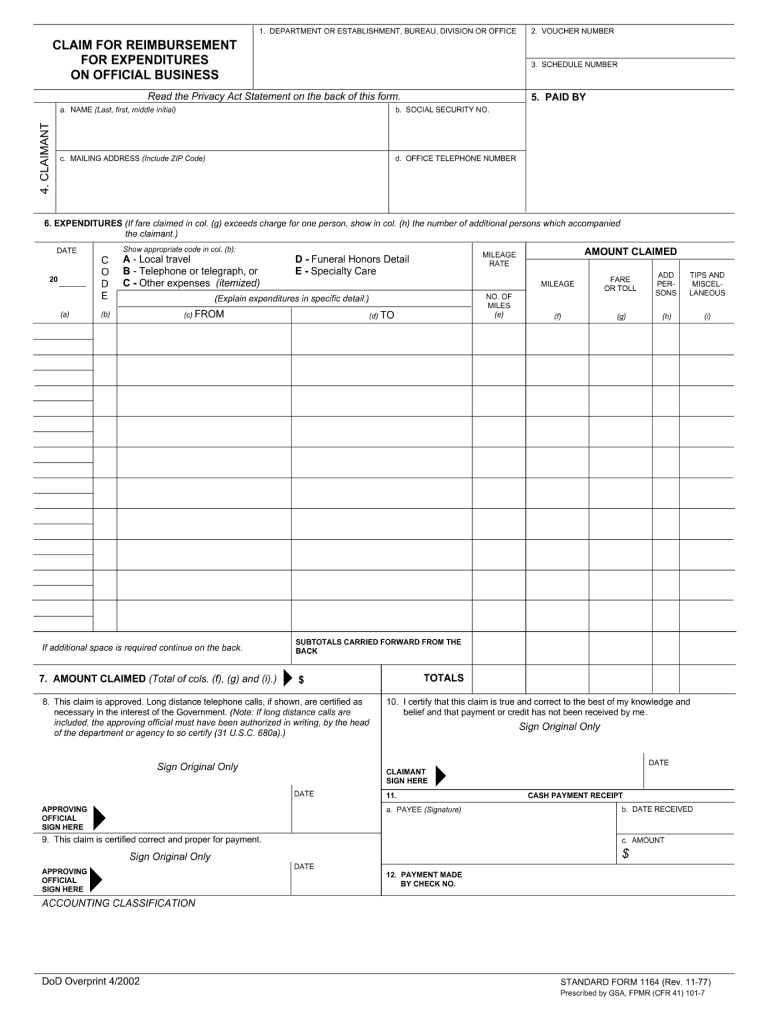
What is GSA SF 1169
The GSA SF 1169 is a financial report used by federal agencies to detail travel and transportation expenses for reimbursement purposes.
pdfFiller scores top ratings on review platforms
Who needs GSA SF 1169?
Explore how professionals across industries use pdfFiller.

GSA SF 1169 is needed by:
-
Federal employees filing for travel reimbursement
-
Government contractors managing travel expenses
-
Financial officers in federal agencies
-
Budget analysts assessing travel costs
-
Auditors reviewing travel expenditure
Comprehensive Guide to GSA SF 1169
What is the GSA SF 1169?
The GSA SF 1169 form is a federal travel form essential for managing financial operations within federal agencies. This form plays a crucial role in reporting official travel and foreign expenses, making it significant for both individuals and organizations. By properly utilizing the GSA SF 1169, users can ensure accurate and compliant financial reporting.
Purpose and Benefits of the GSA SF 1169
The primary purpose of the GSA SF 1169 is to facilitate expense reporting for federal travel. Using this form, individuals can enjoy several benefits, including:
-
Tax compliance for travel-related expenses
-
Eligibility for reimbursements
-
Improved record-keeping of travel budgets
Ultimately, the GSA SF 1169 assists users in managing their travel budgets more effectively.
Who Needs the GSA SF 1169?
The GSA SF 1169 is primarily necessary for employees and contractors of federal agencies, as well as related organizations. Various scenarios warrant its use, such as:
-
Official travel for government purposes
-
Reimbursements of foreign expenses
Recognizing the target audience is vital for ensuring proper compliance and usage of the form.
How to Fill Out the GSA SF 1169 Online
To complete the GSA SF 1169 form electronically, users can follow these step-by-step instructions:
-
Access the GSA SF 1169 form online.
-
Fill in the identifying information and travel details in the designated sections.
-
Review all entries for accuracy before submission.
Common pitfalls to avoid include overloading information, which can lead to confusion. Tips for ensuring accurate completion involve double-checking all provided information prior to finalizing the form.
Common Errors and How to Avoid Them
When completing the GSA SF 1169, users often encounter frequent mistakes, such as:
-
Incorrect financial figures
-
Missing required signatures
To mitigate these errors, it’s crucial to verify all information before submission and ensure compliance with federal regulations governing form completion.
Submission Methods and Requirements for the GSA SF 1169
Once completed, the GSA SF 1169 can be submitted through various methods. Users should consider the following options:
-
Online submission through authorized platforms
-
Mailing the completed form to the appropriate agency
Additionally, certain documents may need to accompany the GSA SF 1169, and users should familiarize themselves with relevant deadlines to avoid delays in processing.
What Happens After You Submit the GSA SF 1169?
After submitting the GSA SF 1169, users can expect a processing timeline that varies by agency. Following submission, users will receive feedback or confirmation, providing reassurance of the application's status. It is advisable to check the status of the submission regularly and follow up if necessary.
Security and Compliance When Handling the GSA SF 1169
Handling the GSA SF 1169 involves securing sensitive personal information. Users should prioritize:
-
Secure storage solutions for completed forms
-
Utilizing platforms that offer encryption and regulatory compliance
Taking these steps ensures that information remains protected while using the GSA SF 1169.
Streamline Your GSA SF 1169 Experience with pdfFiller
pdfFiller offers a user-friendly interface for editing and completing the GSA SF 1169 form, enhancing the overall experience. Key features of pdfFiller include:
-
eSigning capabilities for quick approvals
-
The ability to share completed forms easily
-
Conversion options for different file formats
Users are encouraged to utilize pdfFiller to optimize their document management process, making handling the GSA SF 1169 more efficient.
How to fill out the GSA SF 1169
-
1.Start by visiting pdfFiller and searching for 'GSA SF 1169' in the document search bar.
-
2.Once located, click on the form to open it in the pdfFiller editor, where you can begin filling it out.
-
3.Gather the necessary information such as travel dates, destinations, expenses incurred, and any receipts you may need to reference.
-
4.Use the editing tools to navigate through the form. Click on each field to enter relevant data. Make sure all sections are completed accurately.
-
5.Review the filled form to check for any errors and ensure that all required information has been provided.
-
6.Once you are satisfied with the form’s content, you can save your work in pdfFiller. Click on the save icon, and select the preferred format.
-
7.You can download the form to your device or submit it electronically through the options available in pdfFiller, depending on how you need to deliver it.

What is the purpose of the GSA SF 1169?
The GSA SF 1169 is used by federal agencies to report travel and transportation expenses for reimbursement. It's essential for ensuring accurate financial reporting.
Who is eligible to fill out the GSA SF 1169?
Federal employees who have incurred travel expenses during authorized business trips are eligible to fill out the GSA SF 1169 for reimbursement.
What information do I need to complete the GSA SF 1169?
You will need details like travel dates, locations, the purpose of travel, and itemized expenses including receipts for any costs incurred.
How do I submit the GSA SF 1169 after filling it out?
After completing the GSA SF 1169, you can submit it electronically via pdfFiller or download it and submit it according to your agency's requirements.
Are there any common mistakes to avoid when filling out the form?
Common mistakes include missing fields, incorrect expense amounts, and not including supporting documents like receipts. Double-check your entries before submission.
What is the processing time for GSA SF 1169 submissions?
Processing times for GSA SF 1169 submissions can vary depending on the agency. It's best to check with your agency’s finance department for specific timelines.
Is notarization required for the GSA SF 1169?
No, notarization is not required for the GSA SF 1169. The form is primarily a financial report that requires accurate data submission.
Related Content
Related Forms

Related Catalogs
Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.