Last updated on Apr 10, 2026
FL DFS-F5-DWC-10 free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
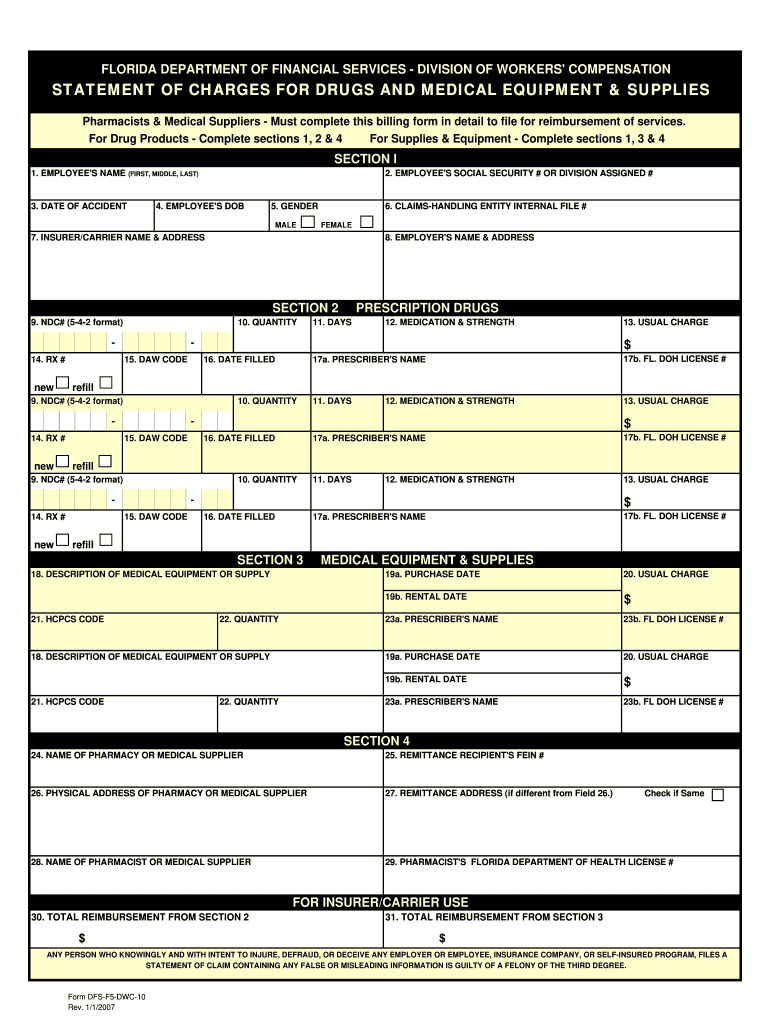
What is FL DFS-F5-DWC-10
The Florida Workers' Compensation Drug and Medical Equipment Billing Form is a medical billing document used by pharmacists and medical suppliers to seek reimbursement for prescription drugs and medical equipment related to workers' compensation claims in Florida.
pdfFiller scores top ratings on review platforms
Who needs FL DFS-F5-DWC-10?
Explore how professionals across industries use pdfFiller.

FL DFS-F5-DWC-10 is needed by:
-
Pharmacists filing for workers' comp reimbursements.
-
Medical suppliers providing equipment to injured employees.
-
Insurance adjusters reviewing reimbursement claims.
-
Healthcare providers assisting with medication management.
-
Workers' compensation claimants needing to verify expenses.
Comprehensive Guide to FL DFS-F5-DWC-10
What is the Florida Workers' Compensation Drug and Medical Equipment Billing Form?
The Florida Workers' Compensation Drug and Medical Equipment Billing Form, known as the DFS-F5-DWC-10, serves as a pivotal resource within Florida's workers' compensation system. This essential form is specifically designed for pharmacists and medical suppliers engaged in providing prescription drugs and medical equipment to injured employees.
Completing the DFS-F5-DWC-10 form accurately is crucial for timely reimbursement processes. By ensuring proper documentation, pharmacists and suppliers can effectively submit claims for reimbursement, thus facilitating smoother transactions in the healthcare landscape.
Purpose and Benefits of the Florida Workers' Compensation Drug and Medical Equipment Billing Form
The primary purpose of the Florida Workers' Compensation Drug and Medical Equipment Billing Form is to streamline the reimbursement process for prescription drugs and medical equipment. Accurate completion of this form significantly impacts the speed and efficiency of reimbursement, benefiting both healthcare providers and injured employees.
-
Facilitates timely reimbursement for services rendered.
-
Reduces the likelihood of claim denials due to incomplete information.
-
Enhances the overall patient experience by providing clarity on treatment costs.
Who Needs the Florida Workers' Compensation Drug and Medical Equipment Billing Form?
This form is primarily needed by pharmacists, medical suppliers, and healthcare providers involved in workers' compensation claims. It serves as an essential documentation tool for anyone submitting claims for reimbursement related to services provided to injured employees.
-
Pharmacists dispensing medication under workers' compensation.
-
Medical suppliers providing necessary equipment for treatment.
-
Healthcare providers seeking reimbursement for medical services rendered.
-
Injured employees receiving care who require assurance of coverage.
How to Fill Out the Florida Workers' Compensation Drug and Medical Equipment Billing Form Online
Filling out the Florida Workers' Compensation Drug and Medical Equipment Billing Form online can be a straightforward process. Start by gathering all required information, such as the employee's name and date of accident. Below is a step-by-step guide to complete the form effectively.
-
Access the DFS-F5-DWC-10 form on a reliable platform.
-
Enter the Employee's Name and Social Security Number accurately.
-
Provide details of the prescription or medical equipment.
-
Double-check entries in the Usual Charge field.
-
Utilize the pdfFiller interface for seamless completion.
Common Mistakes and How to Avoid Them When Filling Out the Form
Accurate completion of the Florida Workers' Compensation Drug and Medical Equipment Billing Form is vital. However, common errors can occur that may delay reimbursement processes. Understanding these pitfalls can help ensure that submissions are error-free.
-
Incorrect Social Security Numbers leading to claim denials.
-
Omitting critical details in the Usual Charge section.
-
Failing to sign and date the form appropriately.
Always double-check your entries to mitigate these issues. Employ validation techniques such as proofreading and using digital tools for accuracy before submission.
Submission of the Florida Workers' Compensation Drug and Medical Equipment Billing Form
Submitting the completed Florida Workers' Compensation Drug and Medical Equipment Billing Form is an important step in the reimbursement process. Understanding available submission methods can facilitate a smooth experience.
-
Submissions can be made online directly through the provider's portal.
-
Alternately, physical copies can be mailed to the appropriate workers' compensation office.
-
Ensure all necessary supporting documents, such as evidence of services provided, are included.
Be aware of submission deadlines and estimated processing times to avoid delays in reimbursement.
Tracking Your Submission and What to Expect After Filing
After submitting the Florida Workers' Compensation Drug and Medical Equipment Billing Form, tracking your submission is crucial for ensuring prompt action. Knowing what to expect after filing can help you navigate the process efficiently.
-
Confirmation of submission can often be received through the online portal.
-
Processing statuses can usually be tracked via the same platform.
-
Expect communications regarding reimbursements or any required corrections within a designated timeframe.
Importance of Security and Compliance When Handling the Florida Workers' Compensation Form
When dealing with sensitive information on the Florida Workers' Compensation Drug and Medical Equipment Billing Form, security and compliance are paramount. Utilizing a secure platform is essential to protect personal data during the submission process.
-
pdfFiller provides robust document security through 256-bit encryption.
-
Complying with both HIPAA and GDPR regulations ensures user trust.
-
Employing best practices when handling sensitive documents is vital to uphold privacy.
How pdfFiller Can Simplify Your Florida Workers' Compensation Billing Process
pdfFiller can greatly enhance the efficiency of filling out and submitting the Florida Workers' Compensation Drug and Medical Equipment Billing Form. The platform offers numerous features designed to support users throughout the entire process.
-
Fillable forms that reduce the likelihood of errors.
-
eSigning options for faster processing.
-
A user-friendly interface that guides users through each step.
Sample Completed Florida Workers' Compensation Drug and Medical Equipment Billing Form
A visual reference can be beneficial when navigating the Florida Workers' Compensation Drug and Medical Equipment Billing Form. A sample completed form can provide clarity on filling out each field.
-
Key areas include the proper completion of essential fields like the Employee's Name and Date of Accident.
-
Highlighted sections illustrate the importance of accuracy and completeness.
-
Focused explanations on any additional details required for successful submission.
How to fill out the FL DFS-F5-DWC-10
-
1.Access the Florida Workers' Compensation Drug and Medical Equipment Billing Form on pdfFiller by searching the official form name in their search bar.
-
2.After you open the PDF, familiarize yourself with the interface, noting where the fillable fields are located on the form.
-
3.Gather necessary information including the employee's name, social security number, date of the accident, prescription details, and provider information before filling out the form.
-
4.Begin completing the form by clicking inside the designated fields using pdfFiller's tools, ensuring you provide accurate and complete information.
-
5.Double-check the entries in each field for accuracy to avoid common mistakes that can delay processing.
-
6.Once all fields are filled, review the form by using pdfFiller’s preview option to ensure clarity and correctness.
-
7.After finalizing your details, utilize the save function on pdfFiller to store your completed form either online or on your device.
-
8.If ready to submit, download the form in your preferred format or use pdfFiller’s emailing features for direct submission to relevant parties.

What are the eligibility requirements for using this form?
This form is intended for pharmacists and medical suppliers submitting reimbursement claims for services provided to injured employees under Florida's workers' compensation system.
Are there deadlines for submitting this billing form?
While specific deadlines are not detailed in the metadata, it's crucial to submit claims promptly within the regulatory timeframes for workers' compensation to ensure reimbursement.
How should I submit the completed Florida Workers' Compensation form?
After completion, you can submit the form by downloading it and mailing it to the relevant insurance provider or using pdfFiller's direct submission options, if available.
What supporting documents are needed when submitting this form?
Usually, you'll need to include copies of invoices and any pertinent medical records that validate the charges for prescription drugs and medical equipment.
What common mistakes should I avoid when filling out this form?
Common errors include inaccurate employee information, missing signatures, and not providing all requested details, leading to delays or denials.
How long does it typically take to process the form once submitted?
Processing times can vary widely based on the insurance provider, but typically expect at least several weeks for reimbursement to be issued after submission.
Can I make changes to the form after I've submitted it?
Once submitted, changes are generally not possible without resubmitting a corrected form. It's best to ensure accuracy before the initial submission.
FL DFS-F5-DWC-10 Form Versions
Related Content
Related Forms



Related Catalogs

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.