Last updated on Apr 10, 2026
Get the free 0938 0214
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
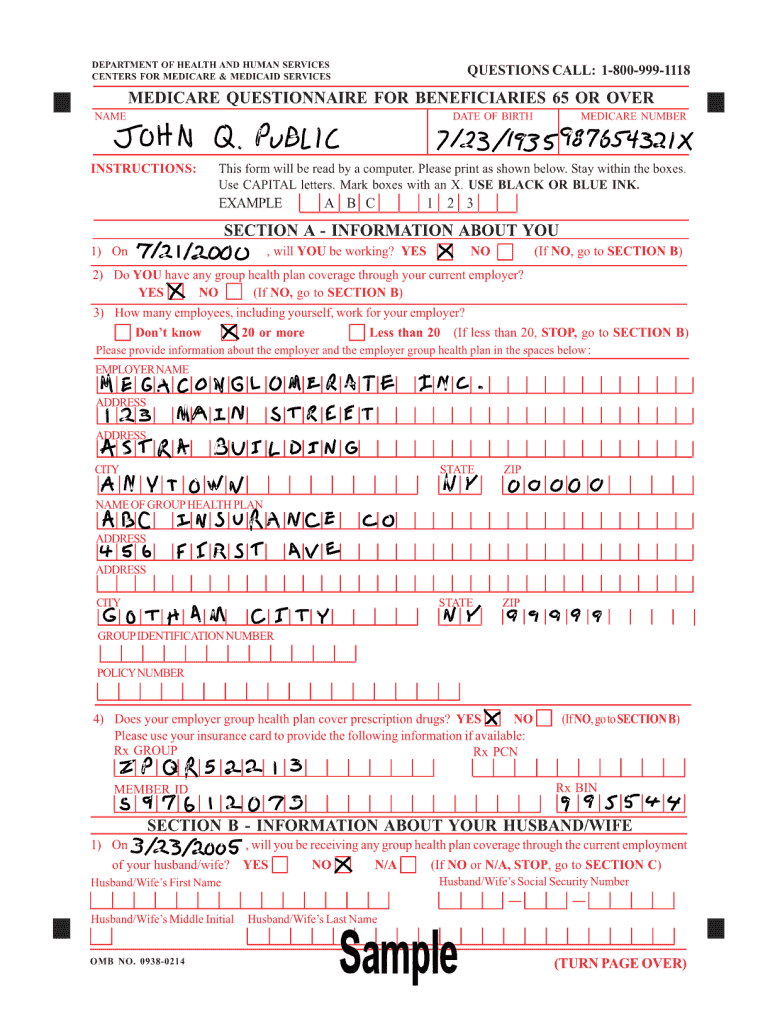
What is 0938 0214
The 0938 0214 is a form used by individuals to submit specific information for official processing or approval.
pdfFiller scores top ratings on review platforms
Who needs 0938 0214?
Explore how professionals across industries use pdfFiller.

0938 0214 is needed by:
-
Individuals applying for government services
-
Nonprofit organizations seeking funding
-
Business professionals submitting applications
-
Legal representatives managing documents
-
Financial advisors assisting clients
Comprehensive Guide to 0938 0214
What is Form 0?
Form 0 is a crucial document used for specific applications, ensuring users maintain compliance with regulations. It is primarily utilized by individuals or businesses in scenarios that require formal documentation, such as tax filings or governmental submissions. Understanding its definition and purpose is essential for those who need to navigate various bureaucratic processes effectively.
Purpose and Benefits of Form 0
The main objective of Form 0 is to facilitate efficient processing of relevant applications. Using this form correctly provides significant benefits, including legal compliance and streamlined procedures. By following the guidelines, users can avoid potential issues and ensure that their submissions are timely and accurate.
Eligibility Criteria for Form 0
Eligibility for Form 0 is determined by specific criteria, ensuring that only qualified individuals or entities can utilize it. Common situations include instances related to tax exemptions or specific governmental benefits, where users must meet certain conditions. Understanding these criteria is vital for proper use of the form.
How to Fill Out Form 0 Online (Step-by-Step)
Filling out Form 0 online involves several clear steps:
-
Access the online form through the designated platform.
-
Gather necessary personal and financial information required for completion.
-
Carefully input data into each section, ensuring accuracy and completeness.
-
Review the form for any errors before submission.
-
Submit the form electronically and save a copy for your records.
Field-by-Field Instructions for Form 0
Each field in Form 0 contains specific instructions regarding the information required:
-
Field 1: Enter your full name as it appears on legal documents.
-
Field 2: Provide your social security number or tax ID.
-
Field 3: Fill in your current address; ensure it matches with other records.
Many users find certain fields challenging; double-checking entered data can prevent common mistakes.
Submission Methods and Where to Submit Form 0
There are several methods to submit your completed Form 0:
-
Online submission through a designated portal.
-
Mailing a physical copy to the appropriate agency for processing.
Always verify the correct address and required postage for mailed submissions to avoid delays.
Consequences of Not Filing or Late Filing Form 0
Failing to file Form 0 on time can lead to various repercussions, including penalties or legal issues. Timely submission is essential for compliance, ensuring users avoid unnecessary complications related to their applications.
How pdfFiller Can Help with Form 0
pdfFiller offers several features that streamline the process of managing Form 0:
-
Edit and modify the form with ease.
-
Create fillable fields for others to complete.
-
Easily eSign and share the document securely.
Utilizing pdfFiller enhances the overall efficiency and security of document management.
Security and Compliance for Form 0
Form 0 is handled with robust security measures to protect user data. pdfFiller employs 256-bit encryption and adheres to regulations such as HIPAA and GDPR, ensuring that all submissions remain confidential and secure throughout the process.
Next Steps After Filing Form 0
After submitting Form 0, users can expect to receive confirmation of their submission. It's also crucial to know how to track the status of the application and make necessary corrections if required, ensuring all details are accurately processed.
Maximize Your Experience with pdfFiller
To further enhance your experience, explore the various features of pdfFiller, which can simplify the form-filling process. Engaging with additional resources available through the platform can also provide valuable insights and tools to assist with document management.
How to fill out the 0938 0214
-
1.To access the 0938 0214 form on pdfFiller, visit the pdfFiller website and use the search feature to find the form by name or number.
-
2.Once you have located the form, click on it to open in the pdfFiller editor, where you can begin filling it out.
-
3.Before starting, gather any necessary information, such as personal identification details, financial information, or relevant documentation that pertains to the form's requirements.
-
4.Navigate through the form fields using your mouse or keyboard tab key. Click on each field to enter text or select options from dropdowns as applicable.
-
5.Make sure to complete all required fields, indicated typically by an asterisk or highlighted area. Read each section carefully to ensure all information is accurate.
-
6.Once you have completed the form, review all entries for any errors or omissions. Use pdfFiller’s review tools to check spelling and formatting.
-
7.After finalizing your information, you can save the form within your pdfFiller account to return to later, or download it directly for your records.
-
8.To submit the form, choose the appropriate submission method as instructed, ensuring you follow any guidance provided on the form regarding delivery methods, such as email or postal service.

Who is eligible to fill out the 0938 0214 form?
Eligibility typically includes individuals applying for certain services, organizations that meet specific criteria, and professionals acting on behalf of clients. Generally, if you need to submit information for review or processing, you may be eligible.
What is the deadline for submitting the 0938 0214 form?
Deadlines vary based on the specific purpose of the form. It is essential to check any relevant guidelines or instructions provided with the form, as late submissions may delay processing.
How can I submit the 0938 0214 form once completed?
You can submit the form either electronically via email as instructed or by mailing a physical copy. Ensure you follow the submission guidelines to avoid delays or rejections.
What supporting documents are needed to accompany the 0938 0214 form?
Supporting documents may include identification, proof of eligibility, or financial records specific to the application process. Always refer to the form instructions for detailed requirements.
What common mistakes should I avoid when filling out the form?
Common mistakes include missing required fields, incorrect information, and failing to double-check entries before submission. Taking your time to review can help prevent these errors.
How long will processing take once I submit the form?
Processing times for the 0938 0214 form can vary based on workload and the nature of the application. Typically, you should allow a few weeks for processing, but urgent requests may be prioritized.
What should I do if I find an error after submitting the 0938 0214 form?
If an error is found after submission, contact the relevant agency immediately to explain the situation. They will provide guidance on how to correct or amend the submitted form.
Related Content
Related Forms


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.