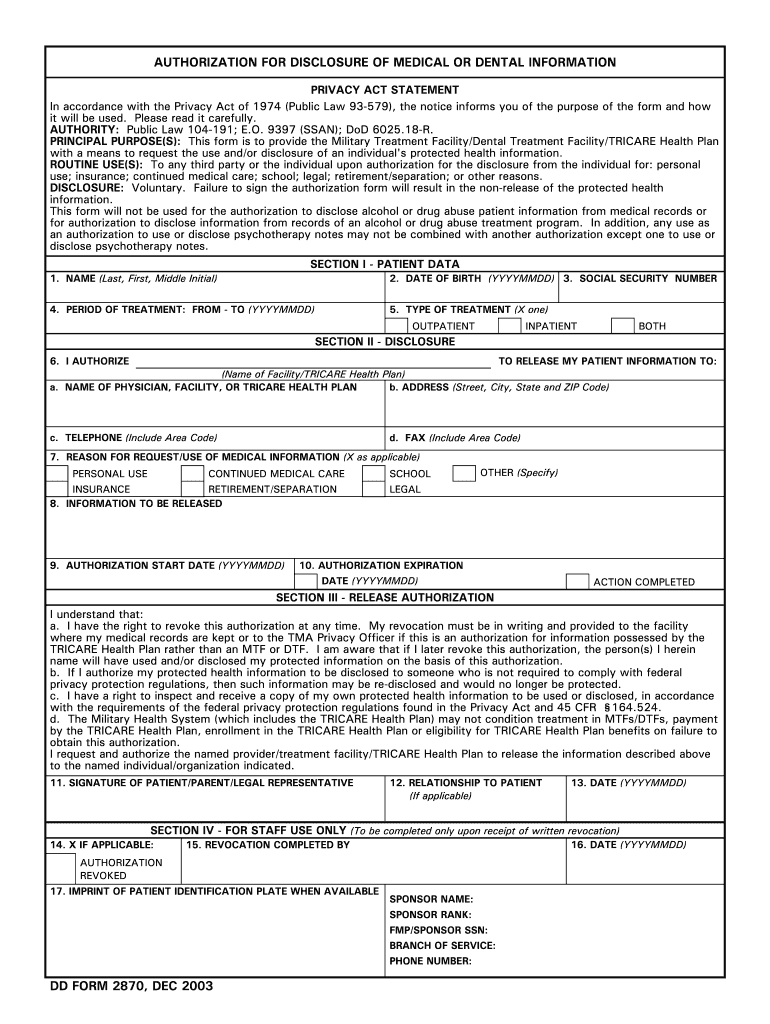



Who needs a DD 2870 Form?
A DD form 2870 is typically submitted by a TRI CARE beneficiary (a military employee, a military retiree, or their defendants) on the request of their provider or contractor. Filling out this form is not mandatory and can be denied.
What is the DD 2870 Form for?
The filled out DD form 2870 (Authorization for Disclosure of Medical or Dental Information) is permission to share individual’s protected health information to a third party or individual upon authorization for the disclosure for several purposes:
- personal use
- insurance
- continued medical care
- school
- legal
- retirement/separation, etc.
Is the DD 2870 Form accompanied by other forms?
There is no need to submit any other forms along with the DD 2870.
When is DD 2870 Form due?
The form’s submission is not regulated by any specific deadlines. However, the applicant must indicate the “Authorization Start Date” and “Authorization Expiration Date”, unless the request will not be processed.
How do I fill out DD 2870 Form?
To be legal, the form must be completed in a comprehensive way and include the following information:
- patient data (name, date of birth, SSN, period and type of treatment)
- disclosure containing name of the facility or Trocar health plan, and necessary information about the party which the — authorization is made to
- reasons for request or use of medical information
- information that is to be released
- authorization start and expiration dates
- signature and date
Where do I send DD 2870 Form?
The completed form should be sent to one of the TRI CARE offices, depending on the beneficiary’s location Harry is a full list of addresses.