
CA DE 2515 2012 free printable template
Show details
(Fold)(Fold)Disability is an illness or injury, either physical
or mental, which prevents customary work.
Disability includes elective surgery, pregnancy,
childbirth, or related medical conditions.DI
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign CA DE 2515
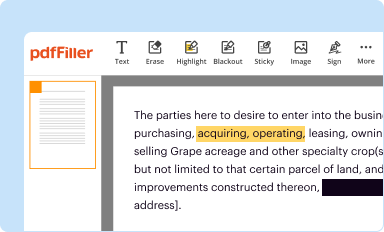
Edit your CA DE 2515 form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
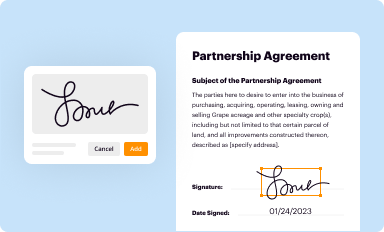
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
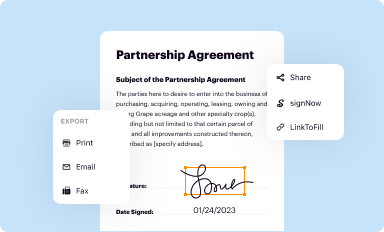
Share your form instantly
Email, fax, or share your CA DE 2515 form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit CA DE 2515 online



Follow the guidelines below to use a professional PDF editor:
1
Log in. Click Start Free Trial and create a profile if necessary.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit CA DE 2515. Rearrange and rotate pages, insert new and alter existing texts, add new objects, and take advantage of other helpful tools. Click Done to apply changes and return to your Dashboard. Go to the Documents tab to access merging, splitting, locking, or unlocking functions.
4
Save your file. Select it from your records list. Then, click the right toolbar and select one of the various exporting options: save in numerous formats, download as PDF, email, or cloud.
Dealing with documents is always simple with pdfFiller.
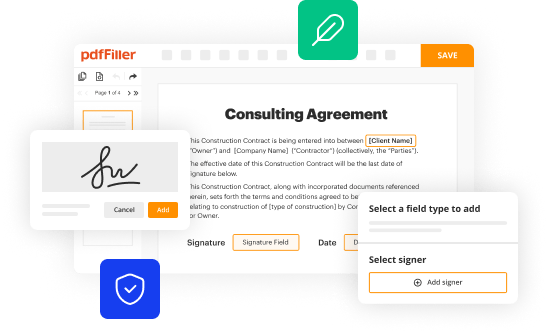
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
CA DE 2515 Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out CA DE 2515
How to fill out CA DE 2515
01
Begin by downloading the CA DE 2515 form from the California Employment Development Department (EDD) website.
02
Fill in your personal information, including your name, address, and Social Security number.
03
Indicate the reason for your claim by checking the appropriate box.
04
Enter the dates for which you are requesting benefits.
05
Provide any requested information regarding your previous employment.
06
Review the completed form for accuracy before submission.
07
Submit the form as instructed, either online or via mail to the specified address on the form.
Who needs CA DE 2515?
01
Individuals who are unable to work due to a medical condition, and are seeking disability benefits in California need to fill out CA DE 2515.
02
Employees needing to claim benefits due to a qualifying disability.
03
Anyone who has a valid physician's certification for their inability to work due to medical reasons.
Fill
form
: Try Risk Free
People Also Ask about
What form does my doctor have to fill out for disability EDD?
For Disability Insurance claims, fill out and sign Part B – Physician/Practitioner's Certificate on the Claim for Disability Insurance (DI) Benefits (DE 2501) form. Mail it in within 49 days from the date your patient's disability begins.
What is DE 2515?
Disability Insurance Provisions Brochure (DE 2515) Rev.
How to fill out a de 2501 form?
To complete a DE 2501 Form you will need to provide the following information: Health Insurance Portability and Accountability Act (HIPAA) Authorization. Social security number. Name. Claimant's Statement. Social security number. EDD customer account number. Physician/Practitioner's Certificate. Patient's SSN.
What is a de2525xx form?
Physician/Practitioner's Supplementary Certificate (DE 2525XX): If your disability will extend beyond the original period established on your claim, have your physician/practitioner complete and submit the DE 2525XX online using SDI Online.
What form does my doctor have to fill out for disability in California?
For Disability Insurance claims, fill out and sign Part B – Physician/Practitioner's Certificate on the Claim for Disability Insurance (DI) Benefits (DE 2501) form. Mail it in within 49 days from the date your patient's disability begins.
Where can I get a DE 2501 form?
You can get a paper Claim for Disability Insurance (DI) Benefits (DE 2501) form by: Ordering a form onlineto have it mailed to you. Getting the form from your licensed health professional or employer. Visiting an SDI Office. Calling 1-800-480-3287 and selecting DI Information option 3 to request a paper form by mail.
Can I download de 2501?
Claim for Disability Insurance (DI) Benefits (DE 2501) – English: You must submit an original form provided by the EDD, either electronically or through US mail. It cannot be downloaded or reproduced.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I edit CA DE 2515 from Google Drive?
By combining pdfFiller with Google Docs, you can generate fillable forms directly in Google Drive. No need to leave Google Drive to make edits or sign documents, including CA DE 2515. Use pdfFiller's features in Google Drive to handle documents on any internet-connected device.
How do I execute CA DE 2515 online?
pdfFiller makes it easy to finish and sign CA DE 2515 online. It lets you make changes to original PDF content, highlight, black out, erase, and write text anywhere on a page, legally eSign your form, and more, all from one place. Create a free account and use the web to keep track of professional documents.
Can I sign the CA DE 2515 electronically in Chrome?
Yes. By adding the solution to your Chrome browser, you may use pdfFiller to eSign documents while also enjoying all of the PDF editor's capabilities in one spot. Create a legally enforceable eSignature by sketching, typing, or uploading a photo of your handwritten signature using the extension. Whatever option you select, you'll be able to eSign your CA DE 2515 in seconds.
What is CA DE 2515?
CA DE 2515 is a form used in California for reporting information regarding contributions to a qualified defined benefit pension plan.
Who is required to file CA DE 2515?
Employers who have a qualified defined benefit pension plan and are reporting contributions to the plan are required to file CA DE 2515.
How to fill out CA DE 2515?
To fill out CA DE 2515, gather all necessary information regarding the defined benefit pension plan and contributions, then complete the form by following the provided instructions, ensuring all required fields are accurately filled.
What is the purpose of CA DE 2515?
The purpose of CA DE 2515 is to collect data on contributions made to defined benefit pension plans to ensure compliance with state regulations and to facilitate proper record-keeping.
What information must be reported on CA DE 2515?
CA DE 2515 must report information such as the employer's details, plan identification, contribution amounts, participant information, and any applicable signature or certification.
Fill out your CA DE 2515 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
CA DE 2515 is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
