ID Case Management Packet free printable template
Show details
For convenience, soldiers may complete and sign a consent form (DD 2870) to release information to Case. Management (phone available from CM, online, or in ...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign dd form 2870
Edit your dd form 2870 form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your dd form 2870 form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing dd form 2870 online



To use the professional PDF editor, follow these steps:
1
Log in. Click Start Free Trial and create a profile if necessary.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit dd form 2870. Rearrange and rotate pages, insert new and alter existing texts, add new objects, and take advantage of other helpful tools. Click Done to apply changes and return to your Dashboard. Go to the Documents tab to access merging, splitting, locking, or unlocking functions.
4
Get your file. Select the name of your file in the docs list and choose your preferred exporting method. You can download it as a PDF, save it in another format, send it by email, or transfer it to the cloud.
Dealing with documents is simple using pdfFiller. Try it right now!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out dd form 2870
How to fill out ID Case Management Packet
01
Gather all necessary personal information, including your name, address, and contact details.
02
Collect relevant documents, such as identification proof, proof of residency, and any required legal documents.
03
Carefully read the instructions provided with the ID Case Management Packet to ensure compliance.
04
Fill out each section of the packet accurately, ensuring that all fields are completed.
05
Review your entries for any mistakes and ensure all supporting documents are included.
06
Submit the completed packet to the appropriate office or agency as indicated in the instructions.
Who needs ID Case Management Packet?
01
Individuals seeking identification services.
02
People applying for benefits that require verified identity.
03
Residents applying for state or federal IDs, such as driver's licenses or ID cards.
04
Anyone involved in a legal process that necessitates identification confirmation.
Fill
form
: Try Risk Free
People Also Ask about
What is Tricare authorization for disclosure of medical information?
Authorization for Disclosure of Medical Information Form This form enables a beneficiary to authorize Health Net Federal Services, LLC (HNFS) or its subcontractor to release his or her medical information to a specified third party, for example, a spouse, relative or law firm.
What is a dd2870 form?
Authorization for Disclosure of Medical or Dental Information (DD Form 2870) Your provider or contractor will use this form is to get your permission to share your protected health information to a third party for personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
What is DD 2870 Authorization for Disclosure of Medical information?
Authorization for Disclosure of Medical or Dental Information (DD Form 2870) Use this form to authorize an individual to release information that is protected under the Federal Privacy Act. This form is not valid to designate a representative for the Appeals process.
What is DD Form 2870 Authorization for Disclosure of medical or Dental information?
Authorization for Disclosure of Medical or Dental Information (DD Form 2870) Use this form to authorize an individual to release information that is protected under the Federal Privacy Act. This form is not valid to designate a representative for the Appeals process.
What is authorization for disclosure of Medical or dental information DD Form 2870?
Authorization for Disclosure of Medical or Dental Information (DD Form 2870) Use this form to authorize an individual to release information that is protected under the Federal Privacy Act. This form is not valid to designate a representative for the Appeals process.
What is a dd2870 used for?
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
How to fill out DD Form 2870 for retirement?
To complete the DD Form 2870, please follow these instructions carefully: Block 1: Patient's name in this block. Block 2: Patient's date of birth in this block. Block 3: Patient's complete social security number in this block. Block 4: Indicate the date(s) of treatment you (the patient) wants released.
How do I fill out a DD Form 2870?
To complete the DD Form 2870, please follow these instructions carefully: Block 1: Patient's name in this block. Block 2: Patient's date of birth in this block. Block 3: Patient's complete social security number in this block. Block 4: Indicate the date(s) of treatment you (the patient) wants released.
What is a DD Form 2870?
Authorization for Disclosure of Medical or Dental Information (DD Form 2870) Your provider or contractor will use this form is to get your permission to share your protected health information to a third party for personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
How to fill out a DD 2870 form?
To complete the DD Form 2870, please follow these instructions carefully: Block 1: Patient's name in this block. Block 2: Patient's date of birth in this block. Block 3: Patient's complete social security number in this block. Block 4: Indicate the date(s) of treatment you (the patient) wants released.
What is DD 2870 authorization for disclosure of medical or dental information?
Authorization for Disclosure of Medical or Dental Information (DD Form 2870) Use this form to authorize an individual to release information that is protected under the Federal Privacy Act. This form is not valid to designate a representative for the Appeals process.
What is DD 2870 authorization for Disclosure of medical information?
Authorization for Disclosure of Medical or Dental Information (DD Form 2870) Use this form to authorize an individual to release information that is protected under the Federal Privacy Act. This form is not valid to designate a representative for the Appeals process.
What is the purpose of DD Form 2870?
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
How long is a dd2870 good for?
Block 10: Expiration date of this authorization (the standard date is one year from the completion date of this form, although patient may choose any date of his/her choice). However, FAHC will NOT accept the release without an expiration date.
How do I fill out a DD Form 2870 for retirement?
To complete the DD Form 2870, please follow these instructions carefully: Block 1: Patient's name in this block. Block 2: Patient's date of birth in this block. Block 3: Patient's complete social security number in this block. Block 4: Indicate the date(s) of treatment you (the patient) wants released.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I modify my dd form 2870 in Gmail?
pdfFiller’s add-on for Gmail enables you to create, edit, fill out and eSign your dd form 2870 and any other documents you receive right in your inbox. Visit Google Workspace Marketplace and install pdfFiller for Gmail. Get rid of time-consuming steps and manage your documents and eSignatures effortlessly.
How do I execute dd form 2870 online?
Easy online dd form 2870 completion using pdfFiller. Also, it allows you to legally eSign your form and change original PDF material. Create a free account and manage documents online.
How do I fill out dd form 2870 using my mobile device?
The pdfFiller mobile app makes it simple to design and fill out legal paperwork. Complete and sign dd form 2870 and other papers using the app. Visit pdfFiller's website to learn more about the PDF editor's features.
What is ID Case Management Packet?
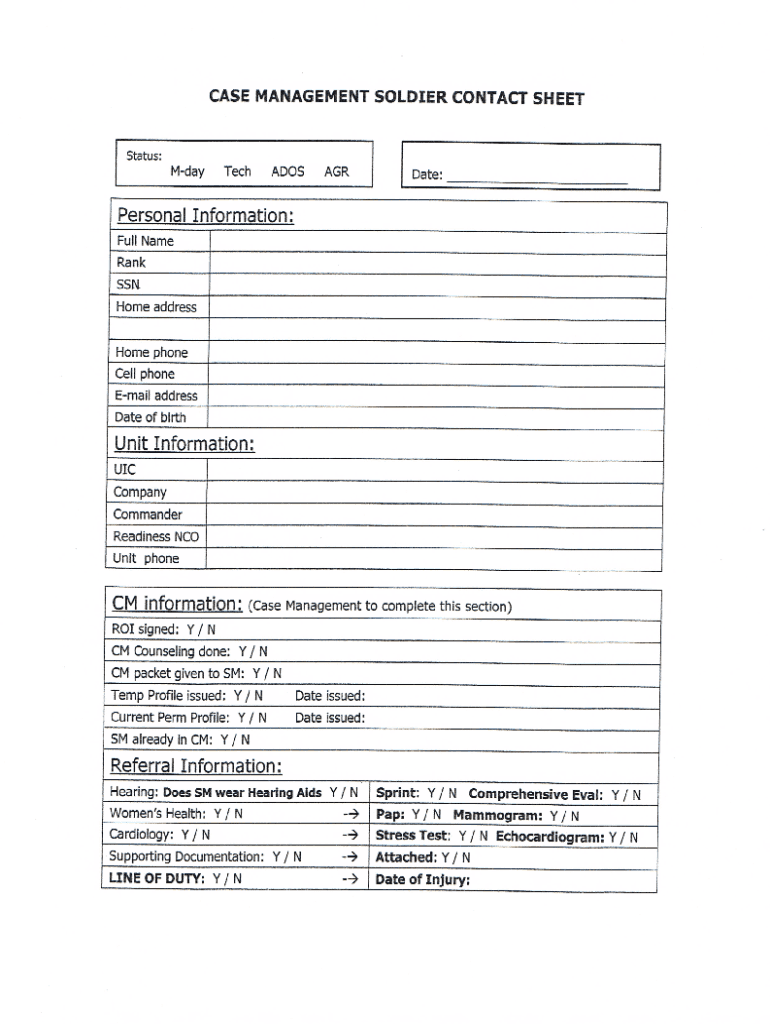
The ID Case Management Packet is a comprehensive document used to collect and manage information regarding individuals with intellectual and developmental disabilities, ensuring that their needs are met and services are effectively delivered.
Who is required to file ID Case Management Packet?
Individuals who are seeking services related to intellectual and developmental disabilities, as well as case managers or service providers on their behalf, are typically required to file the ID Case Management Packet.
How to fill out ID Case Management Packet?
To fill out the ID Case Management Packet, you should follow the provided guidelines, complete all required sections accurately, include necessary documentation, and sign the form where indicated.
What is the purpose of ID Case Management Packet?
The purpose of the ID Case Management Packet is to facilitate the assessment and planning of services for individuals with disabilities, ensuring that their unique needs are addressed and that they receive appropriate support.
What information must be reported on ID Case Management Packet?
The ID Case Management Packet must include personal information, medical history, cognitive and developmental assessments, current services being received, and any specific needs or goals of the individual.
Fill out your dd form 2870 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Dd Form 2870 is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
