Get the free Solicitud de cambio de cobertura para empleados de pequeñas empresas - CA
Show details
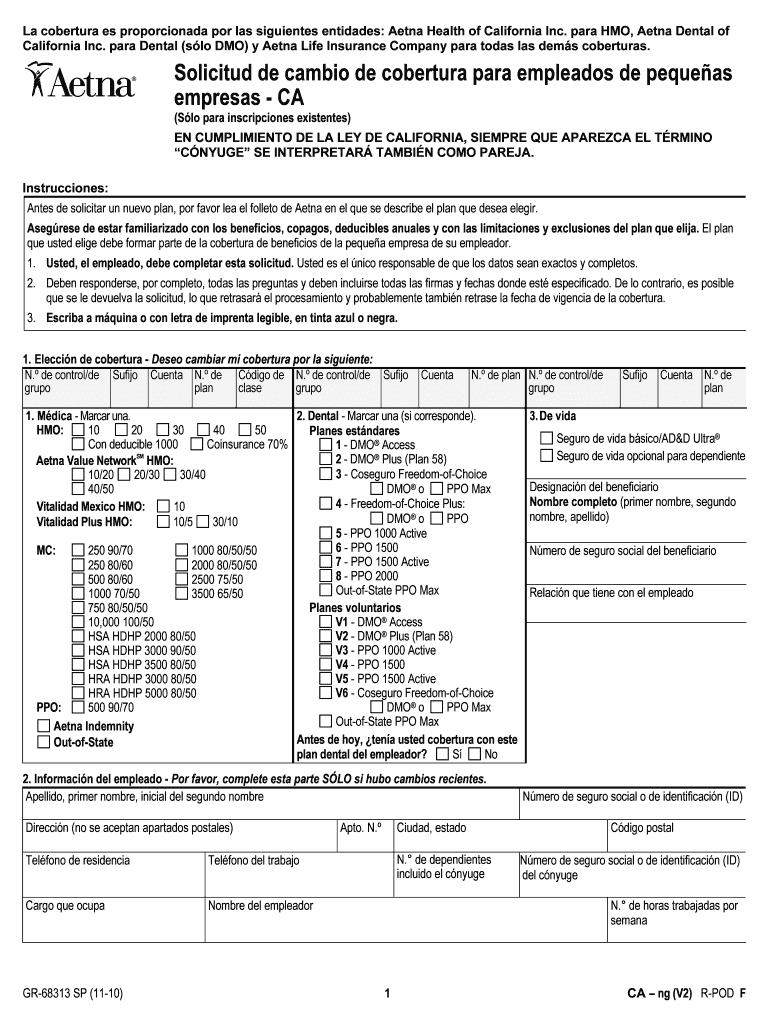
Este documento es una solicitud para que los empleados de pequeñas empresas cambien su cobertura de seguro médico y dental. Incluye secciones para proporcionar información sobre el empleado, elección
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign solicitud de cambio de

Edit your solicitud de cambio de form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your solicitud de cambio de form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing solicitud de cambio de online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit solicitud de cambio de. Rearrange and rotate pages, add new and changed texts, add new objects, and use other useful tools. When you're done, click Done. You can use the Documents tab to merge, split, lock, or unlock your files.
4
Save your file. Choose it from the list of records. Then, shift the pointer to the right toolbar and select one of the several exporting methods: save it in multiple formats, download it as a PDF, email it, or save it to the cloud.
With pdfFiller, dealing with documents is always straightforward.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out solicitud de cambio de

How to fill out Solicitud de cambio de cobertura para empleados de pequeñas empresas - CA
01
Gather necessary information: Collect employee details, current coverage information, and new coverage options.
02
Obtain the Solicitud de cambio de cobertura form: Download or request the form from your insurance provider.
03
Complete the employee information section: Fill in the names, addresses, and other relevant details of employees needing coverage changes.
04
Indicate current coverage: Specify the existing coverage plan each employee is enrolled in.
05
Select new coverage: Choose the new coverage options for each employee as per their needs.
06
Review the form: Double-check all entries for accuracy and completeness.
07
Sign and date: Ensure that the authorized personnel signs and dates the form.
08
Submit the form: Send the completed form to the insurance provider by the required deadline.
Who needs Solicitud de cambio de cobertura para empleados de pequeñas empresas - CA?
01
Small business owners who wish to update their employees' health coverage.
02
Human resources personnel managing employee benefits for small businesses.
03
Employees of small businesses looking to change their current insurance coverage.
Fill
form
: Try Risk Free
People Also Ask about
¿Qué pasa si sus ingresos cambian mientras está con Covered California?
Debe informar los cambios a Covered California en un plazo de 30 días . Para Medi-Cal, debe informarlos en un plazo de 10 días. Para informar los cambios, llame a Covered California al (800) 300-1506 o inicie sesión en su cuenta en línea.
¿Qué ingresos lo descalifican para Covered California?
En la página Historial de Solicitud, haga clic en la pestaña "Inscripción Actual". Revise su inscripción actual. Si alguna información es incorrecta, llame a Covered California inmediatamente al 1-800-300-1506.
¿Cuánto es lo máximo que puedo ganar para calificar para Cover California?
Para informar cambios, llame a Covered California al (800) 300-1506 o inicie sesión en su cuenta en línea. También puede encontrar un agente de seguros con licencia, un asesor de inscripción certificado o un asesor de elegibilidad del condado que le brinde ayuda gratuita en su área.
¿Qué pasa si cometí un error en mi solicitud de Covered California?
En la página Historial de Solicitud, haga clic en la pestaña "Inscripción Actual". Revise su inscripción actual. Si alguna información es incorrecta, llame a Covered California inmediatamente al 1-800-300-1506.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is Solicitud de cambio de cobertura para empleados de pequeñas empresas - CA?
The 'Solicitud de cambio de cobertura para empleados de pequeñas empresas' is a form used in California for small businesses to request changes to their employee health insurance coverage. It allows employers to update or modify existing coverage options for their employees.
Who is required to file Solicitud de cambio de cobertura para empleados de pequeñas empresas - CA?
Small business employers in California who wish to change their employees' health coverage are required to file this form. This includes any business that employs individuals and provide them with health care benefits.
How to fill out Solicitud de cambio de cobertura para empleados de pequeñas empresas - CA?
To fill out the form, employers need to provide specific details such as business information, the intended changes in coverage, employee information, and any required signatures. It’s essential to follow the instructions provided with the form carefully to ensure all necessary information is included.
What is the purpose of Solicitud de cambio de cobertura para empleados de pequeñas empresas - CA?
The purpose of the form is to formally request changes to the health insurance coverage provided to employees of small businesses. This includes adjustments due to changes in business needs, employee numbers, or changes in health plan options.
What information must be reported on Solicitud de cambio de cobertura para empleados de pequeñas empresas - CA?
The form requires information such as the employer's business name, address, and contact details, employee details, current coverage options, the desired changes, and any additional supporting information that may be necessary.
Fill out your solicitud de cambio de online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Solicitud De Cambio De is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
