
Get the free ADA Claim Form
Show details
This document is used to submit dental claims to insurance providers, detailing patient information, treatment specifics, and billing details required for processing claims.
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign ada claim form
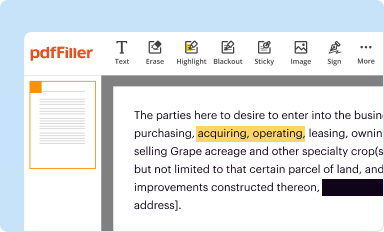
Edit your ada claim form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
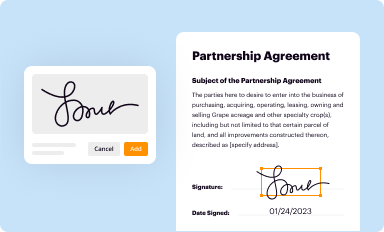
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
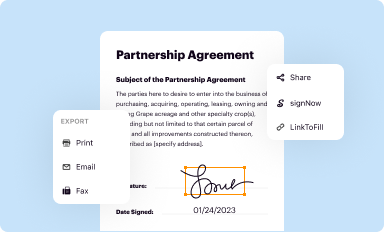
Share your form instantly
Email, fax, or share your ada claim form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
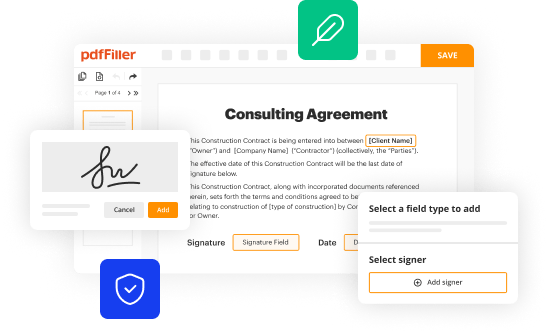
Editing ada claim form online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit ada claim form. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Save your file. Select it from your records list. Then, click the right toolbar and select one of the various exporting options: save in numerous formats, download as PDF, email, or cloud.
With pdfFiller, dealing with documents is always straightforward. Now is the time to try it!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out ada claim form
How to fill out ADA Claim Form
01
Obtain the ADA Claim Form from the appropriate agency or website.
02
Fill in your personal details including name, address, and contact information.
03
Provide details of the incident or condition related to your claim.
04
Include any medical documentation or evidence to support your claim.
05
Complete any additional sections of the form as required.
06
Review the form for accuracy and completeness.
07
Sign and date the form.
08
Submit the form to the designated office or online portal.
Who needs ADA Claim Form?
01
Individuals who believe they have been discriminated against due to a disability.
02
Employees seeking accommodations in the workplace under the ADA.
03
Individuals seeking access to public services or facilities that are not ADA compliant.
04
Anyone who has been denied equal opportunities in housing, employment, or public accommodations due to their disability.
Fill
form
: Try Risk Free
People Also Ask about
How do I submit a corrected ADA claim?
When submitting a corrected claim: Identify the Original Claim: Clearly indicate that the new submission is a corrected claim by referencing the original claim number. Label as “Corrected Claim”: Use the appropriate notation (often “Corrected Claim” or “Resubmission”) on the claim form or in the electronic submission.
What is the submission code for a corrected claim?
XX7 is submitting a replacement/corrected claim. XX8 if submitting a void/cancel of a previous claim.
How to submit a corrected claim on availity?
Claims Correction in Availity Reenter your claim data on the appropriate Claims screen, select Replacement of Prior Claim in the Frequency Type feld, and enter the payer's claim number in the Payer Claim Control Number. Under the Claims & Payment tab is the Claims & Encounters option.
How to send a corrected claim to dental?
Provide Corrected Information: Ensure that all errors are corrected in the new submission, and all necessary information is accurately provided. Include Supporting Documentation: Attach any supporting documents that justify the corrections made, such as notes explaining the change or updated patient records.
What is line 37 on the ADA claim form?
37. I hereby authorize and direct payment of the dental benefits otherwise payable to me, directly to the below named dentist or dental entity.
How to submit a corrected claim electronically?
Electronic Corrected Claim Go to Billing > Bill Insurance. Click on Select Client. Under the Submit Claim section, select the PDF icon for Print & Mail Claim. Next, go to Filing > CMS-1500 and locate the claim. Select the. Under Step 1, select the claims that you want to create the Corrected Claim for.
What claim form is used for dental claims?
The ADA Dental Claim Form, also known as the ADA 2012 form, is a standardized document used for submitting dental insurance claims. It consists of many parts, each serving a specific purpose.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is ADA Claim Form?
The ADA Claim Form is a document used to file claims for benefits under the Americans with Disabilities Act, typically related to disability insurance or health benefits.
Who is required to file ADA Claim Form?
Individuals who are seeking to claim benefits due to a disability that falls under the provisions of the Americans with Disabilities Act are required to file the ADA Claim Form.
How to fill out ADA Claim Form?
To fill out the ADA Claim Form, individuals should carefully follow the instructions provided, ensuring that all fields are completed accurately, providing necessary documentation and signatures as required for the claim.
What is the purpose of ADA Claim Form?
The purpose of the ADA Claim Form is to document and facilitate the process of requesting benefits for individuals who are entitled to protections and accommodations under the Americans with Disabilities Act.
What information must be reported on ADA Claim Form?
The ADA Claim Form typically requires personal identification information, details about the disability, supporting medical information, and any relevant employment or insurance data necessary to process the claim.
Fill out your ada claim form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Ada Claim Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
