Last updated on Mar 23, 2026

Get the free Provider Dispute Resolution Request
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is provider dispute resolution request
The Provider Dispute Resolution Request is a healthcare document used by providers to dispute billing determinations, medical necessity decisions, or contract disagreements with HealthCare Partners Medical Group.
pdfFiller scores top ratings on review platforms
Very easy to use and intuitive uploading and signatures
it is very easy to use and very informative. i would recommend it to everyone.
Who needs provider dispute resolution request?
Explore how professionals across industries use pdfFiller.

Provider dispute resolution request is needed by:
-
Healthcare providers disputing billing claims
-
Medical professionals handling patient cases
-
Administrators within healthcare organizations
-
Billing specialists reviewing claims
-
Legal representatives of healthcare entities
-
Insurance agents managing disputes
Comprehensive Guide to provider dispute resolution request
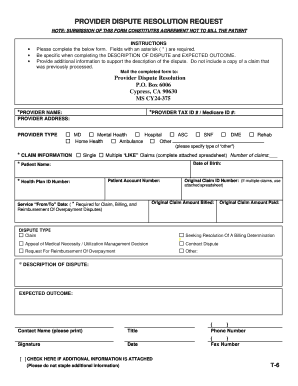
What is the Provider Dispute Resolution Request?
The Provider Dispute Resolution Request form is designed for healthcare providers to formally contest billing determinations and medical necessity decisions. This essential healthcare dispute form is particularly useful in addressing disputes with HealthCare Partners Medical Group, ensuring that providers can articulate their concerns effectively. By utilizing this form, providers can seek resolution and clarity on contested issues related to their services.
Purpose and Benefits of the Provider Dispute Resolution Request
This form serves a crucial role in helping healthcare providers navigate disputes. Utilizing the Provider Dispute Resolution Request can lead to several benefits:
-
Facilitates timely resolution of billing and medical necessity disputes.
-
Supports clear documentation essential for appeals and dispute resolution.
-
Enhances communication between healthcare entities and insurers.
These advantages underscore its necessity for effective dispute management across the healthcare landscape.
Who Needs the Provider Dispute Resolution Request?
The Provider Dispute Resolution Request is intended for eligible healthcare providers who encounter billing disputes. Specific scenarios where this form may be required include:
-
When billing inaccuracies arise after service provision.
-
In cases where medical necessity decisions are questioned.
Additionally, patients should be aware of this form, as it can impact their healthcare experience and the resolution of billing issues related to their care.
When and How to File the Provider Dispute Resolution Request
Filing the Provider Dispute Resolution Request requires attention to specific timelines and procedures:
-
Complete the form accurately, ensuring all relevant information is included.
-
Submit the completed form within the provider's specified deadlines to avoid delays.
Late submissions may result in rejection of the dispute, so adhering to these guidelines is crucial for a successful resolution.
How to Fill Out the Provider Dispute Resolution Request Online (Step-by-Step)
To ensure accurate completion of the Provider Dispute Resolution Request, follow this step-by-step guide:
-
Fill in your Provider NPI and details accurately in the designated fields.
-
Provide the specific Claim Details that pertain to your dispute.
-
Clearly describe the nature of the dispute and your expected outcomes.
Taking these steps will significantly improve the quality and clarity of your submission.
Common Errors and How to Avoid Them
When filling out the Provider Dispute Resolution Request, it's crucial to avoid common mistakes that can lead to rejection:
-
Incomplete fields, especially those requiring critical information like Provider NPI.
-
Failure to provide a clear and concise description of the dispute.
Employing tools like pdfFiller can help minimize these errors and ensure that the form is filled accurately and completely.
How to Sign and Submit the Provider Dispute Resolution Request
Submitting the Provider Dispute Resolution Request requires a clear understanding of signature and submission methods:
-
Digital signatures are often accepted; ensure to validate the requirements.
-
Choose an appropriate submission method, such as electronic submission or mailing the completed form.
When handling sensitive documents like healthcare forms, always ensure that security measures are in place to protect patient information.
What Happens After You Submit the Provider Dispute Resolution Request?
After submitting the Provider Dispute Resolution Request, providers can expect a defined review process:
-
The request will undergo a review, and timelines for responses may vary.
-
Regularly tracking the status of your request is advisable to stay informed of any updates.
If your dispute request is denied or additional information is required, follow the outlined procedures to respond adequately.
How pdfFiller Can Help You with the Provider Dispute Resolution Request
pdfFiller offers several benefits that simplify the process of filling out the Provider Dispute Resolution Request:
-
Users can edit and fill forms quickly and securely with built-in tools.
-
The platform ensures compliance with security standards for healthcare documents.
Using pdfFiller enhances the efficiency of completing and submitting essential forms.
Sample Completed Provider Dispute Resolution Request
To assist users, a sample completed Provider Dispute Resolution Request form demonstrates proper completion:
-
Key sections include fields for Provider NPI, Provider Name, and claim details.
-
Each section should be filled with relevant and accurate information applicable to the dispute scenario.
This example highlights the importance of providing comprehensive information to facilitate effective resolution of disputes.
How to fill out the provider dispute resolution request
-
1.Access pdfFiller and search for 'Provider Dispute Resolution Request'. Open the form to get started.
-
2.Familiarize yourself with the form layout, noting the blank fields and checkboxes provided.
-
3.Before you fill out the form, gather necessary information such as provider details, patient information, and specifics regarding the claim at hand.
-
4.Begin completing the form by filling in your provider information including the Provider NPI and Provider Name.
-
5.Next, enter the patient’s details and provide the relevant claim information with clarity.
-
6.In the dispute section, clearly articulate the reason for the dispute, alongside the expected outcome you hope to achieve.
-
7.Once all fields are filled, review the form carefully to ensure all information is accurate and complete.
-
8.Use the pdfFiller tools to make any needed edits, ensuring all sections are properly completed.
-
9.When satisfied, navigate to the save options to download your completed form, or use the submission features provided by pdfFiller for mailing.

Who is eligible to use the Provider Dispute Resolution Request form?
Healthcare providers who wish to challenge billing or medical necessity decisions made by HealthCare Partners Medical Group are eligible to use this form.
What is the deadline for submitting the Provider Dispute Resolution Request?
While specific deadlines may vary, it is important to submit the form promptly to ensure timely resolution of disputes. Check with HealthCare Partners for any specific time frames.
How can I submit the completed Provider Dispute Resolution Request form?
Once completed, the form should be mailed to the designated address in Torrance, California. Ensure you send it through a reliable postal service for timely processing.
What documents do I need to include with the Provider Dispute Resolution Request?
While not explicitly specified, it's advisable to include any relevant supporting documents or evidence that substantiates your dispute, such as previous correspondence or billing statements.
What are common mistakes to avoid when filling out the form?
Common mistakes include leaving fields blank, providing incorrect or incomplete information, and failing to clearly explain the dispute, which can delay processing.
How long does it take to process the Provider Dispute Resolution Request?
Processing times can vary. Typically, it may take several weeks, so it’s best to follow up with HealthCare Partners if you do not receive updates.
Can I submit the Provider Dispute Resolution Request form online?
The form is intended to be mailed after completion. Check with HealthCare Partners to see if they offer any alternative online submission methods.
Related Forms




Related Catalogs

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.