
NC DHB-5170 2011 free printable template
Show details
Request for Claims Override To: Division of Medical Assistance Claims Analysis Unit From: Telephone Number: County Department of Social Services Date: COMPLETE ALL PERTINENT SECTIONS Recipient: MID:
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign NC DHB-5170
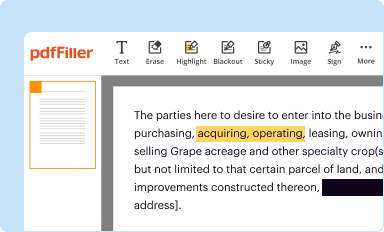
Edit your NC DHB-5170 form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
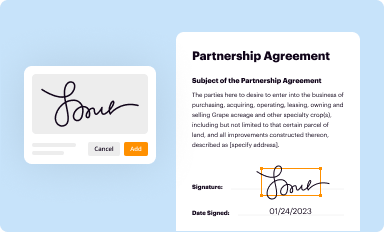
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
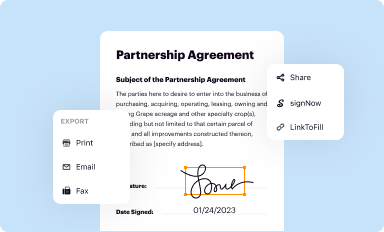
Share your form instantly
Email, fax, or share your NC DHB-5170 form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit NC DHB-5170 online



Follow the guidelines below to use a professional PDF editor:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Simply add a document. Select Add New from your Dashboard and import a file into the system by uploading it from your device or importing it via the cloud, online, or internal mail. Then click Begin editing.
3
Edit NC DHB-5170. Rearrange and rotate pages, add new and changed texts, add new objects, and use other useful tools. When you're done, click Done. You can use the Documents tab to merge, split, lock, or unlock your files.
4
Save your file. Select it from your list of records. Then, move your cursor to the right toolbar and choose one of the exporting options. You can save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud, among other things.
pdfFiller makes working with documents easier than you could ever imagine. Try it for yourself by creating an account!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
NC DHB-5170 Form Versions
Version
Form Popularity
Fillable & printabley
Fill
form
: Try Risk Free
People Also Ask about
What is the look back period for Medicaid in NC?
This means that for the entire 60-month period preceding filing a Medicaid application, the caseworker is going to review any and all financial records from that 60-month period to determine whether the applicant is Medicaid eligible.
What is the phone number for NC Medicaid prior authorization?
How can I submit a prior authorization to a health plan? Urgent: Call 866-799-5318 and follow the prompts. Use the Prior-Auth Check Tool on the website to quickly determine if a service or procedure requires prior authorization. This tool will go live later this summer, before the launch of NC Medicaid Managed care.
What is the look back rule for Medicaid in NC?
Medicaid's Look-Back Rule North Carolina has a 60-month Medicaid Look-Back Period that immediately precedes one's Nursing Home Medicaid or Medicaid Waiver application date. During the “look back”, Medicaid checks all past asset transfers to ensure no assets were sold or gifted under fair market value.
What is the asset limit for Medicaid in NC?
The Medically Needy Asset Limit is $2,000 for an individual and $3,000 for a couple. 2) Asset Spend Down – Persons who have assets over Medicaid's asset limit can still become asset-eligible by reducing countable assets.
What is the asset limit for Medicaid in NC?
North Carolina's Medicaid Resource Limit To qualify for Medicaid in North Carolina, you must have no more than $2,000 in resources (assets like money and property). Some property does not count toward the resource limit.
What is the NC Medicaid utilization review?
The NC Medicaid Drug Utilization Review (DUR) program for outpatient drugs ensures Medicaid recipients receive appropriate, medically necessary prescriptions that are unlikely to result in adverse medical events. NC DUR Board meetings are held quarterly. They are open to the public.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I manage my NC DHB-5170 directly from Gmail?
It's easy to use pdfFiller's Gmail add-on to make and edit your NC DHB-5170 and any other documents you get right in your email. You can also eSign them. Take a look at the Google Workspace Marketplace and get pdfFiller for Gmail. Get rid of the time-consuming steps and easily manage your documents and eSignatures with the help of an app.
Can I sign the NC DHB-5170 electronically in Chrome?
You certainly can. You get not just a feature-rich PDF editor and fillable form builder with pdfFiller, but also a robust e-signature solution that you can add right to your Chrome browser. You may use our addon to produce a legally enforceable eSignature by typing, sketching, or photographing your signature with your webcam. Choose your preferred method and eSign your NC DHB-5170 in minutes.
Can I edit NC DHB-5170 on an Android device?
The pdfFiller app for Android allows you to edit PDF files like NC DHB-5170. Mobile document editing, signing, and sending. Install the app to ease document management anywhere.
What is dma 5170?
dma 5170 is a form used to report certain financial information to regulatory authorities.
Who is required to file dma 5170?
Certain financial institutions and entities are required to file dma 5170.
How to fill out dma 5170?
dma 5170 can typically be filled out online or submitted in physical form with the required information.
What is the purpose of dma 5170?
The purpose of dma 5170 is to provide regulators with important financial data to monitor and regulate certain entities.
What information must be reported on dma 5170?
Information such as financial statements, transaction data, and other relevant financial information must be reported on dma 5170.
Fill out your NC DHB-5170 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
NC DHB-5170 is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
