
Get the free Prescription Advantage Application Form
Show details
This document serves as an application form for the Prescription Advantage program, providing information on eligibility, required documentation, and instruction for applicants in Massachusetts seeking
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign prescription advantage application form
Edit your prescription advantage application form form online
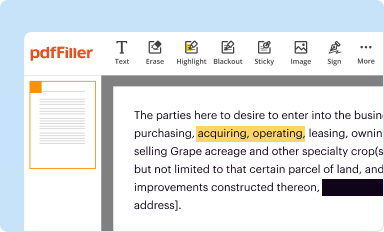
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
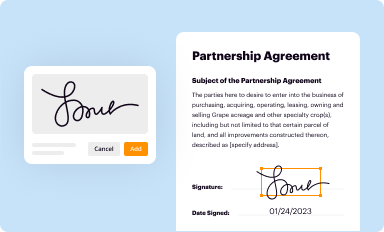
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
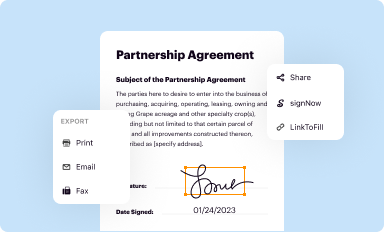
Share your form instantly
Email, fax, or share your prescription advantage application form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing prescription advantage application form online



Follow the steps below to benefit from the PDF editor's expertise:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit prescription advantage application form. Rearrange and rotate pages, add new and changed texts, add new objects, and use other useful tools. When you're done, click Done. You can use the Documents tab to merge, split, lock, or unlock your files.
4
Get your file. When you find your file in the docs list, click on its name and choose how you want to save it. To get the PDF, you can save it, send an email with it, or move it to the cloud.
The use of pdfFiller makes dealing with documents straightforward. Now is the time to try it!
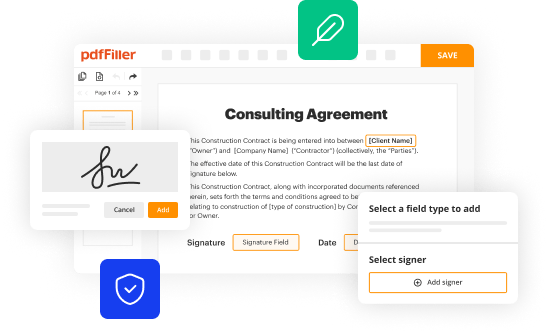
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out prescription advantage application form
How to fill out Prescription Advantage Application Form
01
Obtain the Prescription Advantage Application Form from the official website or a local office.
02
Fill in your personal information, including your name, address, and contact details.
03
Provide your date of birth and Social Security number as required.
04
Indicate your income level and provide documentation if necessary.
05
List any current medications or medical conditions that apply to you.
06
Review the application for accuracy and completeness.
07
Sign and date the form.
08
Submit the application through the specified method (mail, online, in-person).
Who needs Prescription Advantage Application Form?
01
Individuals who are 65 years or older and reside in Massachusetts.
02
Residents who have low income and require assistance with prescription drug costs.
03
People living with specific medical conditions that require ongoing medication.
Fill
form
: Try Risk Free
People Also Ask about
Who is eligible for the Pap program?
Eligibility and enrollment Be a US citizen or legal resident. Have a total household income at or below 400% of the federal poverty level. Must be uninsured, or have Medicare. Note: if you have private or commercial insurance, you are not eligible for the PAP.
What is the prescription advantage program for Medicare?
Medicare Advantage Plan (Part C) A type of Medicare-approved health plan from a private company that you can choose to cover most of your Part A and Part B benefits instead of Original Medicare. It usually also includes drug coverage (Part D). with drug coverage) can use this payment option.
What is the Massachusetts prescription assistance program?
It helps with prescription costs directly, requiring only small deductibles or co-payments until an annual out-of-pocket limit is reached. Once that limit is reached, Prescription Advantage covers the co-payments for the remainder of the plan year.
What is the prescription assistance program?
Patient assistance programs are run by pharmaceutical companies to provide free medications to people who cannot afford to buy their medicine.
What is the 28 day prescription rule in Massachusetts?
It refers to the number of days you may need to wait between refills of 30-day prescriptions that are considered controlled substances. If you have a medication that follows the 28-day rule on a 30-day supply, it means you can get a refill no earlier than 2 days before the 30 days are up.
What are the income guidelines for prescription assistance?
You should contact Social Security for other resource exclusions. What is the income limit? To be eligible for Extra Help, your annual income must be limited to $22,590 for a person or $30,660 for a married couple living together.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is Prescription Advantage Application Form?
The Prescription Advantage Application Form is a form that individuals in need of prescription assistance fill out to enroll in a state-sponsored program that helps cover the costs of prescription medications.
Who is required to file Prescription Advantage Application Form?
Individuals who are eligible for prescription assistance due to age, income, or specific medical needs are required to file the Prescription Advantage Application Form.
How to fill out Prescription Advantage Application Form?
To fill out the Prescription Advantage Application Form, individuals must provide personal information such as name, address, income details, and any relevant medical information. It is important to follow the instructions carefully and ensure all information is accurate before submission.
What is the purpose of Prescription Advantage Application Form?
The purpose of the Prescription Advantage Application Form is to determine eligibility for financial assistance programs that help lower the cost of prescription medications for qualifying individuals.
What information must be reported on Prescription Advantage Application Form?
The information that must be reported on the Prescription Advantage Application Form includes personal identification details, income level, current medications, any insurance coverage, and any other relevant health information.
Fill out your prescription advantage application form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Prescription Advantage Application Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
