
Get the free Delaware Cancer Treatment Program General Prior Authorization Form
Show details
This form is used to request prior authorization for medical and dental procedures related to the Delaware Cancer Treatment Program (DCTP). It requires completion of patient details, diagnosis, procedure
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign delaware cancer treatment program
Edit your delaware cancer treatment program form online
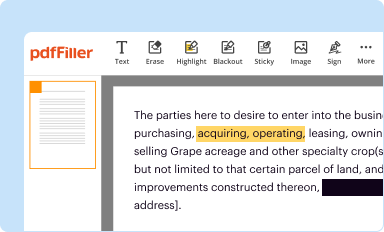
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
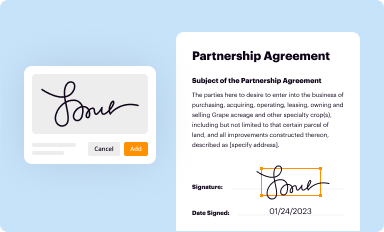
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
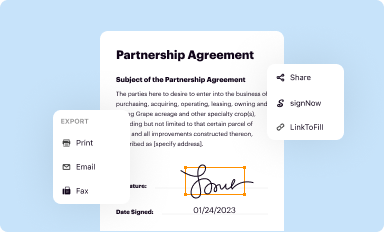
Share your form instantly
Email, fax, or share your delaware cancer treatment program form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit delaware cancer treatment program online



Follow the steps below to benefit from a competent PDF editor:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit delaware cancer treatment program. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Save your file. Select it from your records list. Then, click the right toolbar and select one of the various exporting options: save in numerous formats, download as PDF, email, or cloud.
pdfFiller makes dealing with documents a breeze. Create an account to find out!
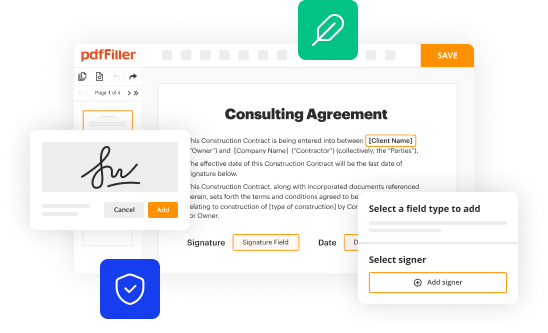
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out delaware cancer treatment program
How to fill out Delaware Cancer Treatment Program General Prior Authorization Form
01
Obtain the Delaware Cancer Treatment Program General Prior Authorization Form from the official website or healthcare provider.
02
Fill in the patient's personal information including name, date of birth, and contact details.
03
Provide the patient's insurance information, including policy number and provider name.
04
Indicate the specific cancer diagnosis and treatment plan as recommended by the healthcare provider.
05
Include any relevant medical history or supporting documentation, such as lab results or previous treatment records.
06
Sign and date the form where indicated, verifying that the information provided is accurate.
07
Submit the completed form to the designated address or fax number as specified in the instructions.
Who needs Delaware Cancer Treatment Program General Prior Authorization Form?
01
Patients diagnosed with cancer who are seeking treatment coverage through the Delaware Cancer Treatment Program.
02
Healthcare providers who are treating patients with cancer and need prior authorization for treatments.
Fill
form
: Try Risk Free
People Also Ask about
What is the Delaware cancer treatment program?
The Delaware Cancer Treatment Program was created to help those who can't afford treatment get the help they need to pay for it. There are also Cancer Care Coordinators available statewide to help guide you through treatment, take care of scheduling, and so much more.
What is the state of Delaware medical assistance program?
Medicaid furnishes medical assistance to eligible low-income families and to eligible aged, blind and/or disabled people whose income is insufficient to meet the cost of necessary medical services.
What is a prior authorization request form?
Prior authorization — also frequently referred to as preauthorization — is a utilization management practice used by health insurance companies that requires certain procedures, tests and medications prescribed by healthcare clinicians to first be evaluated to assess the medical necessity and cost-of-care ramifications
What is the Delaware cancer program?
The Delaware Cancer Treatment Program was created to help those who can't afford treatment get the help they need to pay for it. There are also Cancer Care Coordinators available statewide to help guide you through treatment, take care of scheduling, and so much more.
What does a prior authorization form do?
Prior authorization requires your doctor or provider to obtain approval from your health plan before providing health care services or prescribing prescription drugs. Without prior authorization, your health plan may not pay for your treatment or medication.
Why does Delaware have such high cancer rates?
Although rural Sussex County's cancer death rate is higher than the other two counties (except for lung cancer), and Delaware has only a few more cancers per population than the national average, industrial toxins commonly continue to be blamed for the State's high cancer mortality rate.
What do you get for free if you have cancer?
The Cancer Card Xchange: Distributes gift cards to cancer patients for groceries, transportation, and other essentials. Cancer Alliance of Help & Hope: Provides financial assistance through gift cards. Hope Chest: Offers gift cards for groceries, gas, and other necessities to cancer patients.
What happens if you don't get prior authorization?
What is a prior authorization? Insurance companies use prior authorizations to determine medical necessity before a patient's treatment can begin. A prior authorization can be required for anything from prescription drugs to life-saving surgeries.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is Delaware Cancer Treatment Program General Prior Authorization Form?
The Delaware Cancer Treatment Program General Prior Authorization Form is a document required to obtain prior approval for coverage of cancer treatment services under the Delaware Cancer Treatment Program.
Who is required to file Delaware Cancer Treatment Program General Prior Authorization Form?
The form must be filed by healthcare providers or facilities seeking reimbursement for the cancer treatment services provided to eligible patients under the program.
How to fill out Delaware Cancer Treatment Program General Prior Authorization Form?
To fill out the form, healthcare providers should accurately complete all required fields, including patient information, treatment details, and provider credentials, and submit it to the appropriate reviewing authority.
What is the purpose of Delaware Cancer Treatment Program General Prior Authorization Form?
The purpose of the form is to ensure that cancer treatment services are medically necessary and qualify for financial assistance under the Delaware Cancer Treatment Program.
What information must be reported on Delaware Cancer Treatment Program General Prior Authorization Form?
The form must report patient demographics, diagnosis codes, anticipated treatment plans, provider information, and any supporting documentation that demonstrates the medical necessity of the treatment.
Fill out your delaware cancer treatment program online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Delaware Cancer Treatment Program is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
