Get the free HEALTH INSURANCE SELECTION FORM - nymc
Show details
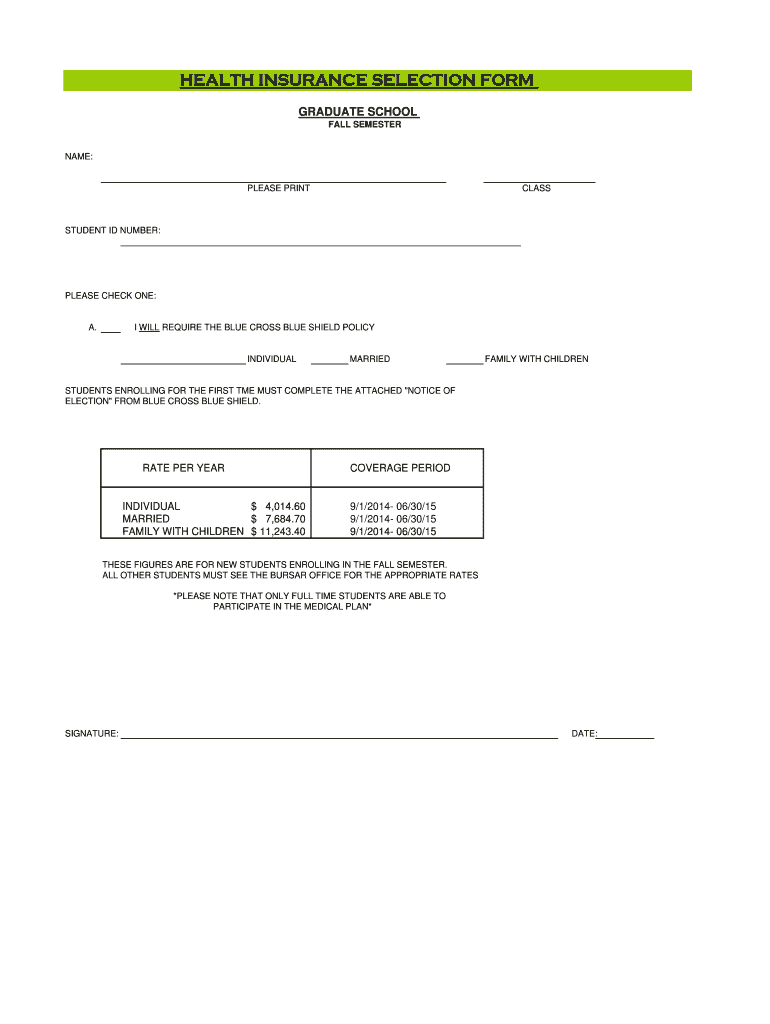
This form is used by graduate students to select their health insurance plan for the fall semester, providing options for individual, married, or family coverage under the Blue Cross Blue Shield policy.
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign health insurance selection form

Edit your health insurance selection form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your health insurance selection form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing health insurance selection form online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Log in. Click Start Free Trial and create a profile if necessary.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit health insurance selection form. Rearrange and rotate pages, add new and changed texts, add new objects, and use other useful tools. When you're done, click Done. You can use the Documents tab to merge, split, lock, or unlock your files.
4
Get your file. Select the name of your file in the docs list and choose your preferred exporting method. You can download it as a PDF, save it in another format, send it by email, or transfer it to the cloud.
pdfFiller makes dealing with documents a breeze. Create an account to find out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out health insurance selection form

How to fill out HEALTH INSURANCE SELECTION FORM
01
Obtain the HEALTH INSURANCE SELECTION FORM from your employer or insurance provider.
02
Read the instructions on the form carefully before filling it out.
03
Provide your personal information, including your name, address, date of birth, and social security number.
04
Select your preferred health insurance plan from the available options.
05
Complete any additional questions regarding dependents, coverage levels, and other relevant details.
06
Review your completed form for accuracy and completeness.
07
Sign and date the form as required.
08
Submit the form according to the provided instructions, ensuring you keep a copy for your records.
Who needs HEALTH INSURANCE SELECTION FORM?
01
Anyone who is eligible for health insurance through their employer or insurance provider.
02
Employees enrolling in a new health insurance plan during open enrollment.
03
Individuals who have experienced a qualifying life event that allows them to change their health insurance coverage.
04
Dependents of employees who require health insurance coverage.
Fill
form
: Try Risk Free
People Also Ask about
Can foreigners buy health insurance in the USA?
New immigrants navigate many changes when they come to the United States, and health insurance coverage can be intimidating. Fortunately, the Affordable Care Act (ACA) provides access to health insurance for non-US citizens who are lawfully present in the United States.
Why do I have to pay back my health insurance tax credit?
When you file your taxes, if your income is less than what you told us on your application, you may receive a credit or refund. If your income is more than what you told us on your application, you may have to repay some or all of the advanced premium tax credits that you got.
Do I need Form 1095-B to file taxes?
Form 1095-B is not required to file your state or federal taxes and you may self‑attest to your health coverage without it. You should get a Form 1095-B in the mail by January 31 following the reported tax year.
Who is required to issue Form 1095-B?
Health insurance issuers and carriers must file Form 1095-B for most health insurance coverage, including individual market coverage and insured coverage sponsored by employers.
How do I fill out a health insurance claim form?
Typical sections of a claim form: Personal information like your name, address and date of birth. Insurance information such as a policy and group number. Reason for your visit including background information about your condition. Provider information including the doctor's name and address.
How does the health care tax credit affect my tax return?
The credit is “refundable” because, if the amount of the credit is more than the amount of your tax liability, you will receive the difference as a refund. If you owe no tax, you can get the full amount of the credit as a refund.
What is a 1095-B form used for health insurance?
Form 1095-B is an Internal Revenue Service (IRS) document that may be used as proof that a person had qualifying health care coverage that counts as Minimum Essential Coverage (MEC) during a tax year.
What is a health insurance verification form?
An insurance verification form is a document that's used by businesses like car dealerships, healthcare facilities, and dental offices to determine whether a person has insurance coverage. Last updated May 12th, 2025.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is HEALTH INSURANCE SELECTION FORM?
The HEALTH INSURANCE SELECTION FORM is a document used by individuals to select and enroll in a health insurance plan, indicating their choice of coverage.
Who is required to file HEALTH INSURANCE SELECTION FORM?
Typically, employees who are eligible for health insurance benefits through their employer are required to file the HEALTH INSURANCE SELECTION FORM during the enrollment period.
How to fill out HEALTH INSURANCE SELECTION FORM?
To fill out the HEALTH INSURANCE SELECTION FORM, individuals should provide personal information, select their desired coverage options, and sign the form as required. It's important to follow the specific instructions provided with the form.
What is the purpose of HEALTH INSURANCE SELECTION FORM?
The purpose of the HEALTH INSURANCE SELECTION FORM is to formalize an individual's choice of a health insurance plan and to ensure that they receive the appropriate benefits.
What information must be reported on HEALTH INSURANCE SELECTION FORM?
The HEALTH INSURANCE SELECTION FORM typically requires personal details such as name, address, and date of birth, as well as the selection of specific coverage options and any dependents to be included.
Fill out your health insurance selection form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Health Insurance Selection Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
