Get the free HEALTH INSURANCE INFORMATION AND SELECTION FORM
Show details
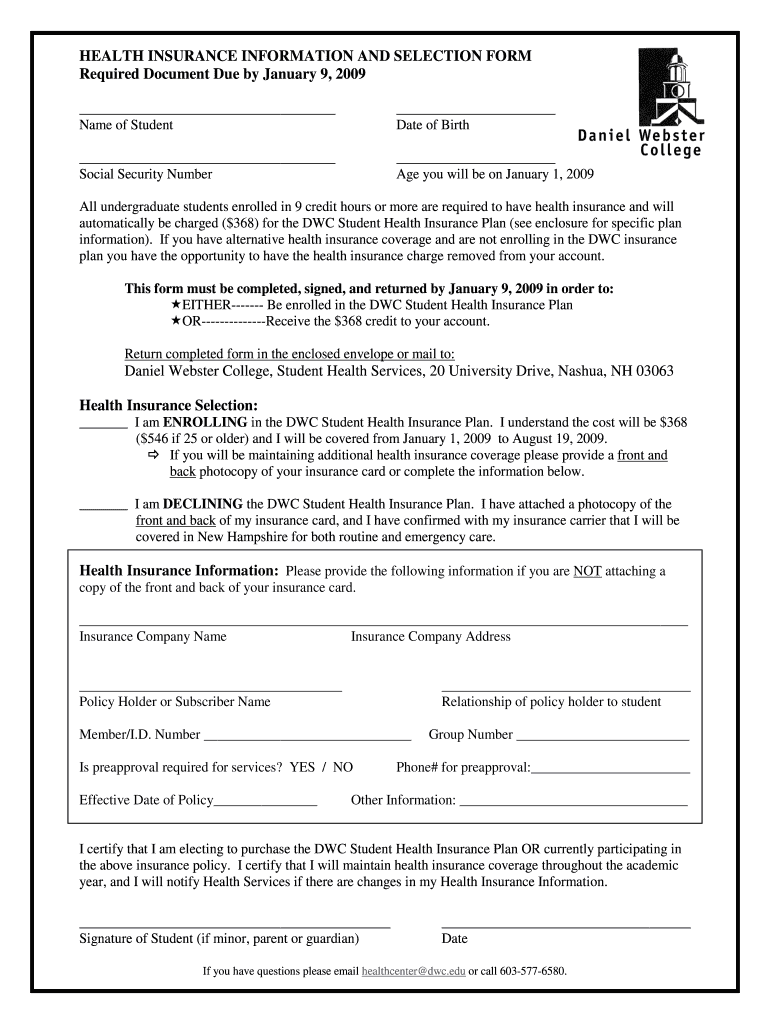
This form is required for undergraduate students to declare their enrollment in the DWC Student Health Insurance Plan or to provide proof of alternative health insurance coverage. It must be completed
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign health insurance information and
Edit your health insurance information and form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your health insurance information and form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing health insurance information and online



To use our professional PDF editor, follow these steps:
1
Register the account. Begin by clicking Start Free Trial and create a profile if you are a new user.
2
Simply add a document. Select Add New from your Dashboard and import a file into the system by uploading it from your device or importing it via the cloud, online, or internal mail. Then click Begin editing.
3
Edit health insurance information and. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Save your file. Choose it from the list of records. Then, shift the pointer to the right toolbar and select one of the several exporting methods: save it in multiple formats, download it as a PDF, email it, or save it to the cloud.
With pdfFiller, it's always easy to work with documents. Try it out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out health insurance information and
How to fill out HEALTH INSURANCE INFORMATION AND SELECTION FORM
01
Begin by reading the instructions provided on the form carefully.
02
Enter your personal details in the required fields, including your name, address, and contact information.
03
Provide your date of birth and social security number as requested.
04
Fill in your employment information, including employer name and address.
05
Indicate your desired health insurance plan choices by marking the appropriate boxes.
06
Include any dependent information if you are enrolling family members under your plan.
07
Review all the information you've entered for accuracy.
08
Sign and date the form at the designated section.
09
Submit the form as instructed, either online or via mail.
Who needs HEALTH INSURANCE INFORMATION AND SELECTION FORM?
01
Individuals seeking health insurance coverage.
02
Employees enrolling in employer-sponsored health plans.
03
Students applying for health insurance through educational institutions.
04
Families looking to include dependents in health insurance plans.
Fill
form
: Try Risk Free
People Also Ask about
How to fill out an insurance claim?
Steps for filing an auto insurance claim Location, date, and time of accident. Name, address, phone number, and insurance policy number for all involved in the accident. Weather conditions. Photo(s) of the damaged vehicle(s) Copies of the police and/or accident reports, if applicable.
What are the 4 most common health insurance plans?
Some popular health insurance policy options are: Preferred provider organization (PPO) plans. Health maintenance organization (HMO) plans. Point of service (POS) plans. Exclusive provider organization (EPO) plans.
Does everyone with health insurance get a 1095?
Will I get at least one form? Maybe. If you were enrolled in health coverage during the year, you should receive a Form 1095-A, 1095-B, or 1095-C. In addition, if you were an employee of an employer that was an applicable large employer during the year, you may receive a Form 1095-C.
What is a MC 216 form?
What is mc216? Beneficiaries who became eligible for Medi-Cal coverage based upon the Affordable Care Acts ACA Modified Adjusted Gross Income MAGI will receive Medi-Cal Renewal Form MC 216. Households with both MAGI and non-MAGI beneficiaries will receive one 1 or more forms sent in one 1 or two 2 packets.
How do I fill out a health insurance claim form?
Typical sections of a claim form: Personal information like your name, address and date of birth. Insurance information such as a policy and group number. Reason for your visit including background information about your condition. Provider information including the doctor's name and address.
What is the first step in completing a claim form?
Top CMS-1500 Form Mistakes Mental Health Providers Make — and How to Avoid Them Mismatched or Incomplete Client Demographics. Missing or Invalid Diagnosis Codes (ICD-10) Incorrect CPT Codes or Modifier Usage. Inaccurate NPI, Tax ID, or Rendering Provider Info. Incorrect Place of Service (POS) Code.
How do you fill out a health insurance claim form?
Typical sections of a claim form: Personal information like your name, address and date of birth. Insurance information such as a policy and group number. Reason for your visit including background information about your condition. Provider information including the doctor's name and address.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is HEALTH INSURANCE INFORMATION AND SELECTION FORM?
The HEALTH INSURANCE INFORMATION AND SELECTION FORM is a document used to provide details regarding an individual's health insurance coverage options and selections. It is typically used in employer-sponsored health insurance plans or during enrollment periods.
Who is required to file HEALTH INSURANCE INFORMATION AND SELECTION FORM?
Individuals who are enrolling in a health insurance plan, whether it's through an employer, government program, or marketplace, are required to file the HEALTH INSURANCE INFORMATION AND SELECTION FORM.
How to fill out HEALTH INSURANCE INFORMATION AND SELECTION FORM?
To fill out the HEALTH INSURANCE INFORMATION AND SELECTION FORM, individuals should provide personal information such as their name, contact details, and dependent information, select their preferred health insurance plan, and provide any required documentation or verification as specified in the instructions.
What is the purpose of HEALTH INSURANCE INFORMATION AND SELECTION FORM?
The purpose of the HEALTH INSURANCE INFORMATION AND SELECTION FORM is to collect necessary information from individuals to facilitate the enrollment and selection process for health insurance coverage, ensuring that all pertinent health insurance choices are documented.
What information must be reported on HEALTH INSURANCE INFORMATION AND SELECTION FORM?
The information that must be reported on the HEALTH INSURANCE INFORMATION AND SELECTION FORM typically includes the individual's personal identification details, employment status, health coverage preferences, dependents' information, and any prior health coverage details if applicable.
Fill out your health insurance information and online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Health Insurance Information And is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
