
Get the free Monthly Payment Notice for the Skilled Nursing Facility Quality Assurance Fee - dhcs ca
Show details
This document serves as a notification for administrators of Free-Standing Skilled Nursing Facilities Level B regarding the Medi-Cal Quality Assurance Fee program, detailing payment instructions,
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign monthly payment notice for
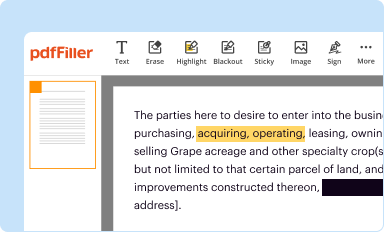
Edit your monthly payment notice for form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
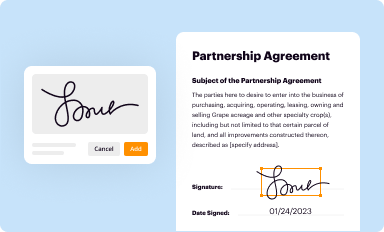
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
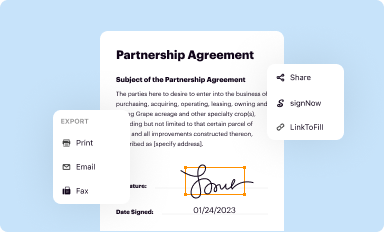
Share your form instantly
Email, fax, or share your monthly payment notice for form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit monthly payment notice for online



To use the professional PDF editor, follow these steps below:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit monthly payment notice for. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Save your file. Select it from your list of records. Then, move your cursor to the right toolbar and choose one of the exporting options. You can save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud, among other things.
pdfFiller makes dealing with documents a breeze. Create an account to find out!
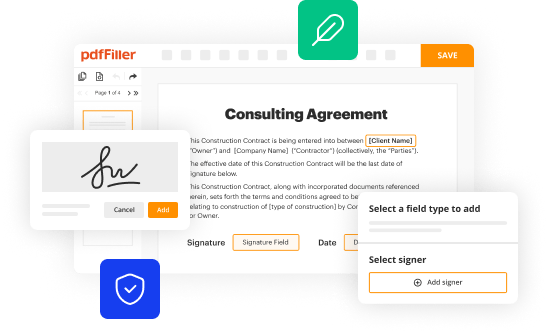
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out monthly payment notice for
How to fill out Monthly Payment Notice for the Skilled Nursing Facility Quality Assurance Fee
01
Obtain the Monthly Payment Notice form from the appropriate regulatory agency.
02
Fill in the facility's name and address at the top of the form.
03
Enter the reporting period for which the payment is being made.
04
Calculate the total number of patient days for the reporting period.
05
Fill in the applicable rate per patient day as specified by the agency.
06
Multiply the total patient days by the rate to determine the total fee amount.
07
Complete any additional required sections, such as contact information for the facility administrator.
08
Sign and date the form where indicated.
09
Submit the form by the deadline specified by the agency, along with any required payment.
Who needs Monthly Payment Notice for the Skilled Nursing Facility Quality Assurance Fee?
01
All skilled nursing facilities operating within the jurisdiction that are required to pay the Quality Assurance Fee.
Fill
form
: Try Risk Free
People Also Ask about
What is a bill type 181?
181 - admit to discharge. 182 - 1st sequential. 183 - cont sequential.
What is the bill type for SNF claims?
Use appropriate covered type of bill (TOB): 211, 212, 213 or 214 for SNF. 181, 182, 183 or 184 for swing bed (SB). Note: TOBs 210 or 180 should not be used for benefits exhaust claims.
What is SNF payment services?
SKILLED NURSING FACILITY. SERVICES PAYMENT SYSTEM. Beneficiaries who need short-term skilled care (nursing or rehabilitation services) on an inpatient basis following a hospital stay of at least three days are eligible to receive covered services in skilled nursing facilities (SNFs).
Is SNF covered by Medicare A or B?
Part A covers inpatient hospital stays, skilled nursing facility care, hospice care, and some home health care. A nursing facility with the staff and equipment to give skilled nursing care and, in most cases, skilled rehabilitative services and other related health services.
What is CMS-1500 bill type?
The CMS-1500 form is the standard claim form used by a non-institutional provider or supplier to bill Medicare carriers and durable medical equipment regional carriers (DMERCs) when a provider qualifies for a waiver from the Administrative Simplification Compliance Act (ASCA) requirement for electronic submission of
How do skilled nursing facilities get paid?
Typically, Medicare will cover a portion of the costs, and the patient's private insurance will cover the remainder. In some cases, Medicaid may also cover a portion of the costs. Ultimately, it is important to work with the skilled nursing facility to determine who is responsible for payment.
What is the bill type for a skilled nursing facility?
Type of Bill By Facility Type of BillFacility Type 022X Skilled Nursing - Inpatient (Medicare Part B Only) 023X Skilled Nursing - Outpatient 028X Skilled Nursing - Swing Beds 032X Home Health Services Under A Plan of Treatment (Effective On 10/1/13)19 more rows • Dec 9, 2023
Why is skilled nursing so expensive?
Labor cost a lot of money, nurses, cooks, cleaning staff and all the others it takes to keep it running. The building and upkeep too and laundry and food. More skills needed the more it cost to keep residents. Doctors and RNs are more expensive than CNAs for example.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is Monthly Payment Notice for the Skilled Nursing Facility Quality Assurance Fee?
The Monthly Payment Notice for the Skilled Nursing Facility Quality Assurance Fee is a document used by skilled nursing facilities to report and pay their quality assurance fees to the state. This fee is intended to fund various healthcare programs and ensure quality standards in skilled nursing facilities.
Who is required to file Monthly Payment Notice for the Skilled Nursing Facility Quality Assurance Fee?
All skilled nursing facilities that are licensed and operate within the state are required to file the Monthly Payment Notice for the Skilled Nursing Facility Quality Assurance Fee.
How to fill out Monthly Payment Notice for the Skilled Nursing Facility Quality Assurance Fee?
To fill out the Monthly Payment Notice, skilled nursing facilities must provide information such as the facility name, license number, reporting month, total number of patient days, and the calculated quality assurance fee. Facilities should follow the guidelines provided by the state authority for proper completion.
What is the purpose of Monthly Payment Notice for the Skilled Nursing Facility Quality Assurance Fee?
The purpose of the Monthly Payment Notice is to ensure that skilled nursing facilities contribute to the financial resources needed to support quality care standards and programs within the state, thereby enhancing the overall quality of care provided to residents.
What information must be reported on Monthly Payment Notice for the Skilled Nursing Facility Quality Assurance Fee?
The information that must be reported includes the skilled nursing facility's name, license number, reporting month, total patient days for the month, quality assurance fee rate, and total fee owed for the period.
Fill out your monthly payment notice for online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Monthly Payment Notice For is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
