
Get the free Authorization for Hospital Discharge - okdhs
Show details
Form 04FE008E is used by the emergency foster care contractor when a child is discharged from a hospital setting directly into emergency foster care with written authorization from Department of Human
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign authorization for hospital discharge
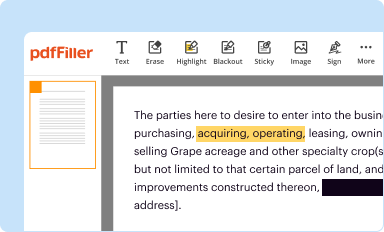
Edit your authorization for hospital discharge form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
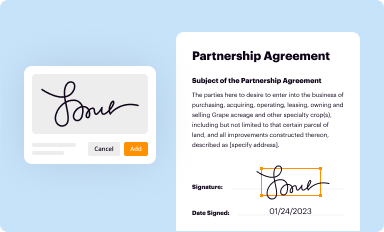
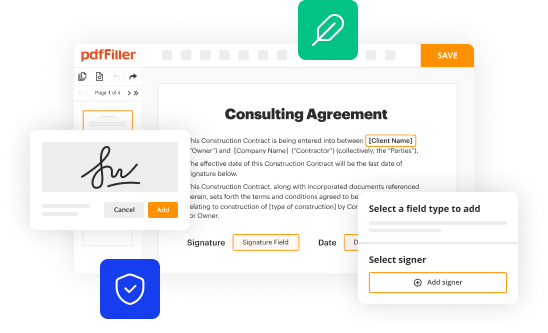
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
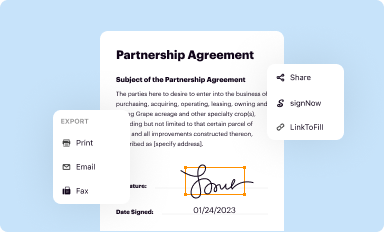
Share your form instantly
Email, fax, or share your authorization for hospital discharge form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit authorization for hospital discharge online



Use the instructions below to start using our professional PDF editor:
1
Check your account. It's time to start your free trial.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit authorization for hospital discharge. Replace text, adding objects, rearranging pages, and more. Then select the Documents tab to combine, divide, lock or unlock the file.
4
Save your file. Choose it from the list of records. Then, shift the pointer to the right toolbar and select one of the several exporting methods: save it in multiple formats, download it as a PDF, email it, or save it to the cloud.
pdfFiller makes working with documents easier than you could ever imagine. Try it for yourself by creating an account!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out authorization for hospital discharge
How to fill out Authorization for Hospital Discharge
01
Obtain the Authorization for Hospital Discharge form from the hospital or your healthcare provider.
02
Fill out the patient's personal information, including their name, date of birth, and hospital ID number.
03
Specify the date of discharge on the form.
04
Provide the name and contact details of the designated person authorized to receive discharge information.
05
Check any necessary boxes to indicate consent for information sharing related to the discharge process.
06
Review the completed form for accuracy and completeness.
07
Sign and date the form where indicated, confirming your consent and understanding.
08
Submit the form to the hospital’s administrative office or discharge planner.
Who needs Authorization for Hospital Discharge?
01
Patients who are being discharged from a healthcare facility.
02
Family members or caregivers who are involved in the discharge process.
03
Healthcare providers needing consent to share patient information during discharge.
04
Insurance companies, if required for authorization or coverage purposes.
Fill
form
: Try Risk Free
People Also Ask about
What is an authorization for treatment?
Prior authorization is the approval from your health insurance that may be required for a service, treatment, or prescription to be covered by your plan if it's not an emergency.
What is authorization in medical terms?
Authorization in medical billing refers to the process wherein the payer authorizes to cover the prescribed services before the services are rendered.
How do I write a self-discharge letter from the hospital?
I, _ (Patient) take full responsibility for discharging myself from hospital. The possible consequences have been explained to me by _ (Doctor) and I fully understand that my action is contrary to medical advice.
What is the purpose of an authorization form?
By signing the authorization, an individual is giving consent to have their health information used or disclosed for the reasons stated on the authorization. Any use or disclosure by the covered entity or business associate must be consistent with what is stated on the form.
What's the difference between consent and authorization?
Voluntary: Consent is optional, and patients can choose to provide or withhold it. In contrast, authorization is mandatory for certain activities. Specificity: Authorization requires detailed information, including the exact nature of the disclosure and who will receive it, making it more specific than consent.
What is a hospital discharge in English?
A discharge occurs whenever a patient leaves hospital upon completion of treatment, signing out against medical advice, transferring to another healthcare institution, or on death. A discharge includes inpatients or day cases and healthy newborn babies should also be included.
What is a patient authorization?
Authorization is the act of permitting access or approval to ensure that a treatment, medication, or procedure is approved before it is administered to your patient. This process protects patient safety and helps maintain compliance with legal and billing standards.
How do you write an authorization to release information?
Content for a valid authorization includes: The name of the person or entity authorized to make the request (usually the patient) The complete name of the person or entity to receive the protected health information (PHI) A specific description of the information to be used or disclosed, including the dates of service.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is Authorization for Hospital Discharge?
Authorization for Hospital Discharge is a formal permission granted by a patient or their representative that allows the hospital to proceed with the discharge process after evaluating that the patient is medically stable and ready to leave the hospital.
Who is required to file Authorization for Hospital Discharge?
The hospital staff, typically a healthcare provider or discharge planner, is required to file the Authorization for Hospital Discharge, often involving the patient or their legal representative's consent.
How to fill out Authorization for Hospital Discharge?
To fill out the Authorization for Hospital Discharge, a healthcare provider must include the patient's information, the reason for discharge, confirmation of the patient's medical condition, and obtain signatures from the patient or their representative.
What is the purpose of Authorization for Hospital Discharge?
The purpose of Authorization for Hospital Discharge is to ensure that patients are safely transitioned from hospital care to home or another care setting while protecting their legal rights and ensuring compliance with healthcare regulations.
What information must be reported on Authorization for Hospital Discharge?
The information that must be reported on Authorization for Hospital Discharge includes the patient's name, date of birth, diagnosis, discharge date, instructions for follow-up care, and any medications prescribed, as well as the signatures of the patient or their representative.
Fill out your authorization for hospital discharge online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Authorization For Hospital Discharge is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
